

Cerebral blood flow decrease as an early pathological mechanism in Alzheimer's disease
- PMID: 32865691
- PMCID: PMC7666276
- DOI: 10.1007/s00401-020-02215-w
Cerebral blood flow decrease as an early pathological mechanism in Alzheimer's disease
Abstract
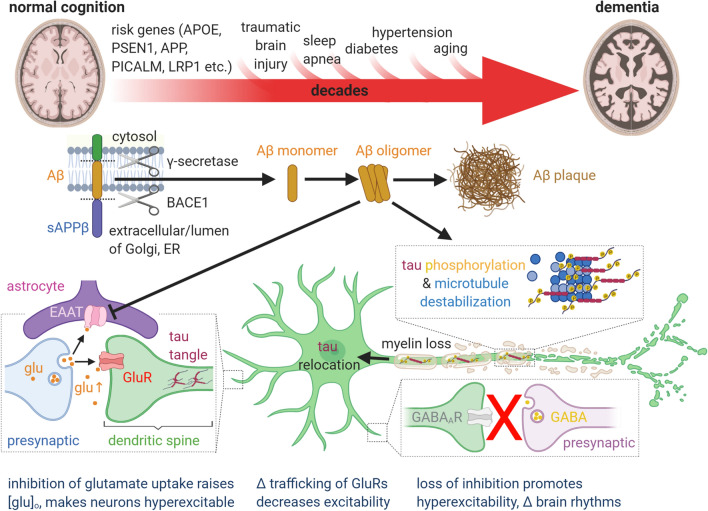
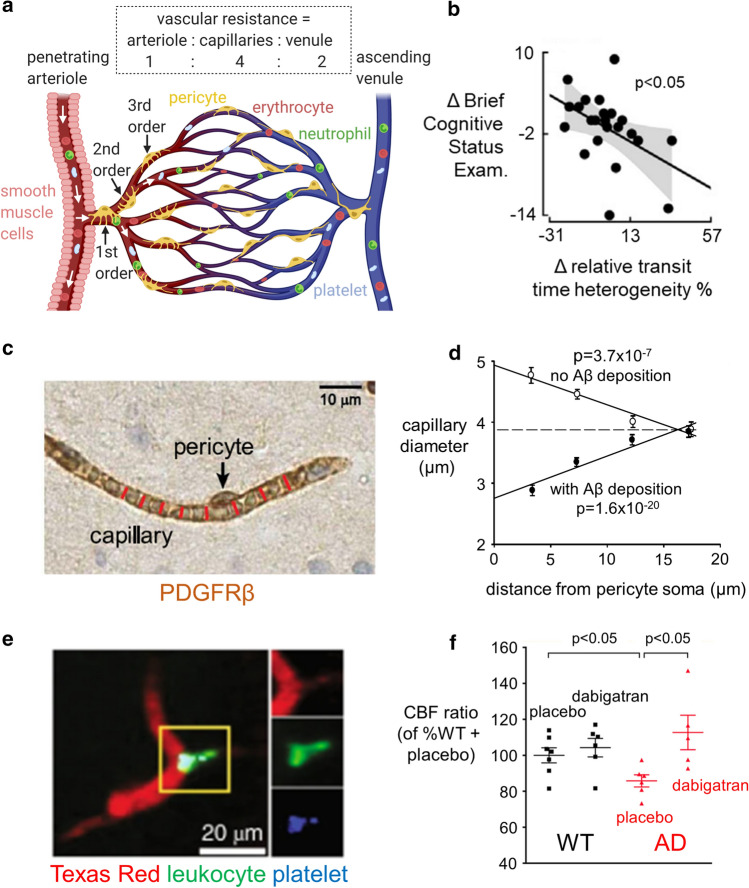
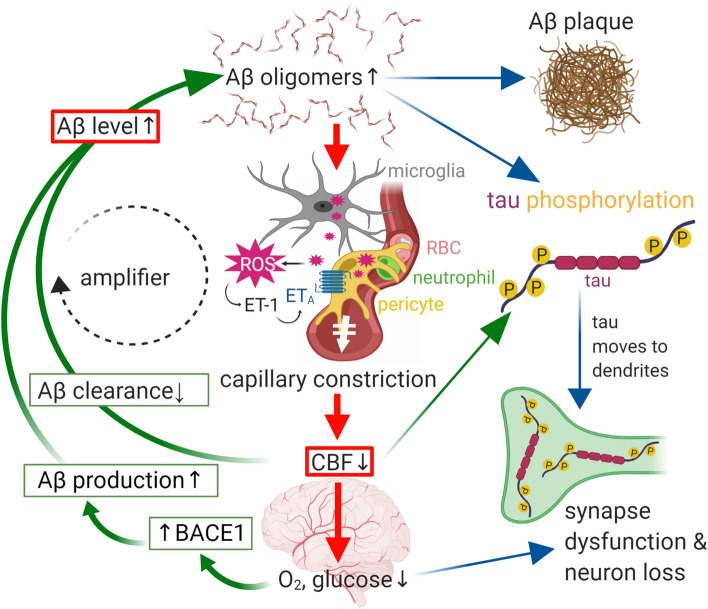
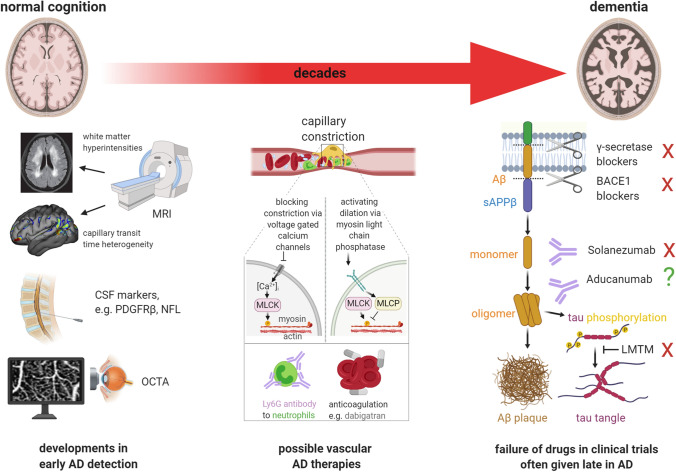
Therapies targeting late events in Alzheimer's disease (AD), including aggregation of amyloid beta (Aβ) and hyperphosphorylated tau, have largely failed, probably because they are given after significant neuronal damage has occurred. Biomarkers suggest that the earliest event in AD is a decrease of cerebral blood flow (CBF). This is caused by constriction of capillaries by contractile pericytes, probably evoked by oligomeric Aβ. CBF is also reduced by neutrophil trapping in capillaries and clot formation, perhaps secondary to the capillary constriction. The fall in CBF potentiates neurodegeneration by upregulating the BACE1 enzyme that makes Aβ and by promoting tau hyperphosphorylation. Surprisingly, therefore, CBF reduction may play a crucial role in driving cognitive decline by initiating the amyloid cascade itself, or being caused by and amplifying Aβ production. Here, we review developments in this area that are neglected in current approaches to AD, with the aim of promoting novel mechanism-based therapeutic approaches.
Keywords: Alzheimer’s; Amyloid β; Capillary; Cerebral blood flow; Neutrophil; Pericyte.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
