

Incorporating Magnetic Resonance Imaging and Biomarkers in Active Surveillance Protocols - Results From the Prospective Stockholm3 Active Surveillance Trial (STHLM3AS)
- PMID: 32866231
- PMCID: PMC8096373
- DOI: 10.1093/jnci/djaa131
Incorporating Magnetic Resonance Imaging and Biomarkers in Active Surveillance Protocols - Results From the Prospective Stockholm3 Active Surveillance Trial (STHLM3AS)
Abstract
Background: Active surveillance (AS) for men with low-risk prostate cancer (PC) can lead to patient morbidity and healthcare overutilization. The aim of this study was to evaluate an AS protocol using the Stockholm3 test and magnetic resonance imaging (MRI) to reduce biopsy intensity.
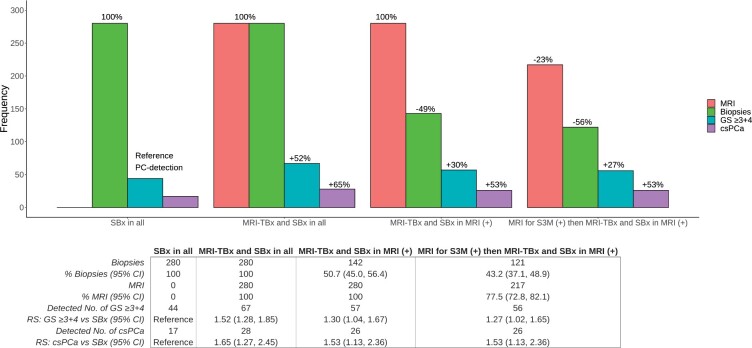
Methods: We conducted a prospective multicenter study of 280 invited men from a contemporary screening study (STHLM3), with Gleason Score (GS) 3 + 3 PC on a current AS protocol. Patients underwent prostate-MRI and blood sampling for analysis of the Stockholm3 test including protein biomarkers, genetic variants, and clinical variables to predict risk of GS ≥3 + 4 PC followed by systematic biopsies and targeted biopsies (for Prostate Imaging Reporting and Data System version 2 ≥3 lesions) in all men. Primary outcomes were reclassification to GS ≥3 + 4 PC and clinically significant PC (csPCa), including unfavorable intermediate risk PC or higher based on National Comprehensive Cancer Network guidelines.
Results: Adding MRI-targeted biopsies to systematic biopsies increased sensitivity of GS ≥3 + 4 PC compared with systematic biopsies alone (relative sensitivity [RS] = 1.52, 95% confidence interval [CI] = 1.28 to 1.85). Performing biopsies in only MRI positive increased sensitivity of GS ≥3 + 4 PC (RS = 1.30, 95% CI = 1.04 to 1.67) and reduced number of biopsy procedures by 49.3% while missing 7.2% GS ≥3 + 4 PC and 1.4% csPCa. Excluding men with negative Stockholm3 test reduced the number of MRI investigations at follow-up by 22.5% and biopsies by 56.8% while missing 6.9% GS ≥3 + 4 PC and 1.3% csPCa.
Conclusion: Including MRI and targeted/systematic biopsies in the follow-up for men on AS increased sensitivity of PC reclassification. Incorporation of risk prediction models including biomarkers may reduce the need for MRI use in men with low-risk PC.
© The Author(s) 2020. Published by Oxford University Press.
Figures

References
-
- Mohler JL, Antonarakis ES, Armstrong AJ, et al.Prostate Cancer, Version 2.2019, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2019;17(5):479–505. - PubMed
-
- Sanda MG, Cadeddu JA, Kirkby E, et al.Clinically localized prostate cancer: AUA/ASTRO/SUO Guideline. Part I: risk stratification, shared decision making, and care options. J Urol. 2018;199(3):683–690. - PubMed
-
- Mottet N., Cornford P., van den Bergh RCN. et al. EAU Guidelines: Prostate Cancer. 2019. https://uroweb.org/guideline/prostate-cancer/. Published. 2019. Accessed June 17, 2020.
-
- Hamdy FC, Donovan JL, Lane JA, et al.10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N Engl J Med. 2016;375(15):1415–1424. - PubMed
-
- Klotz L, Vesprini D, Sethukavalan P, et al.Long-term follow-up of a large active surveillance cohort of patients with prostate cancer. J Clin Oncol. 2015;33(3):272–277. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
