

The peroxisomal disorder spectrum and Heimler syndrome: Deep phenotyping and review of the literature
- PMID: 32866347
- PMCID: PMC8117942
- DOI: 10.1002/ajmg.c.31823
The peroxisomal disorder spectrum and Heimler syndrome: Deep phenotyping and review of the literature
Abstract
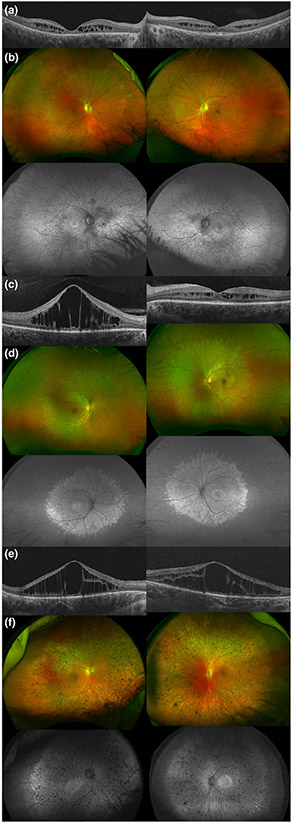
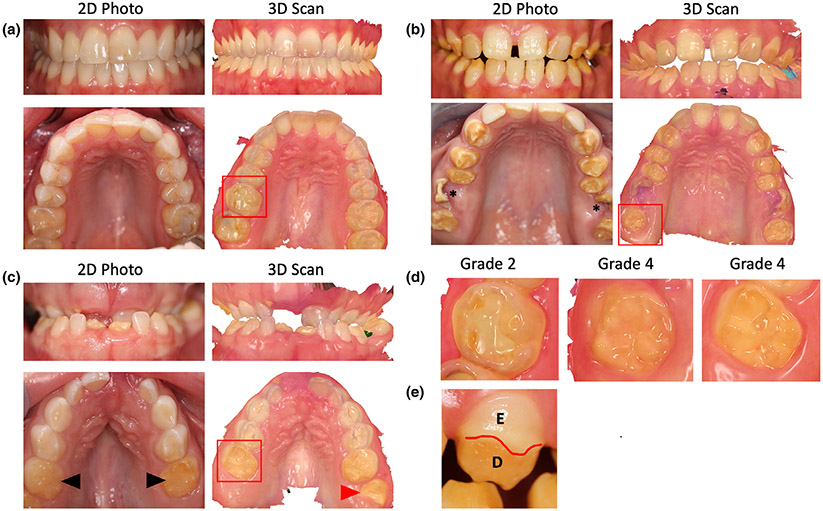
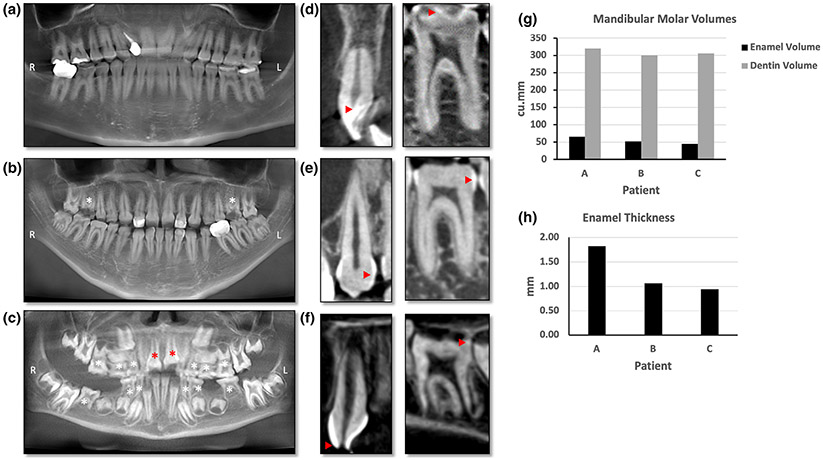
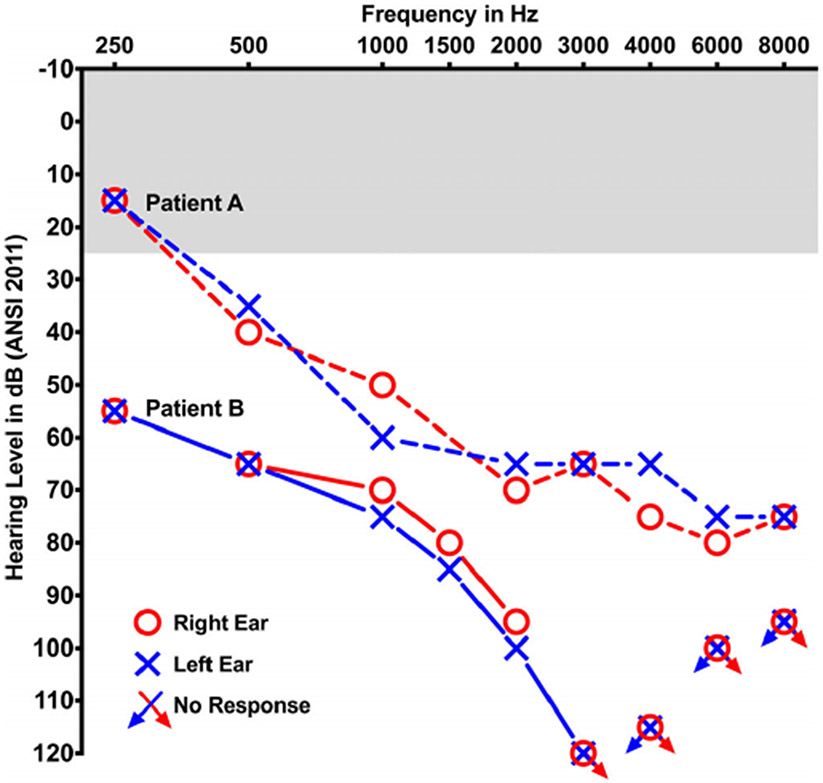
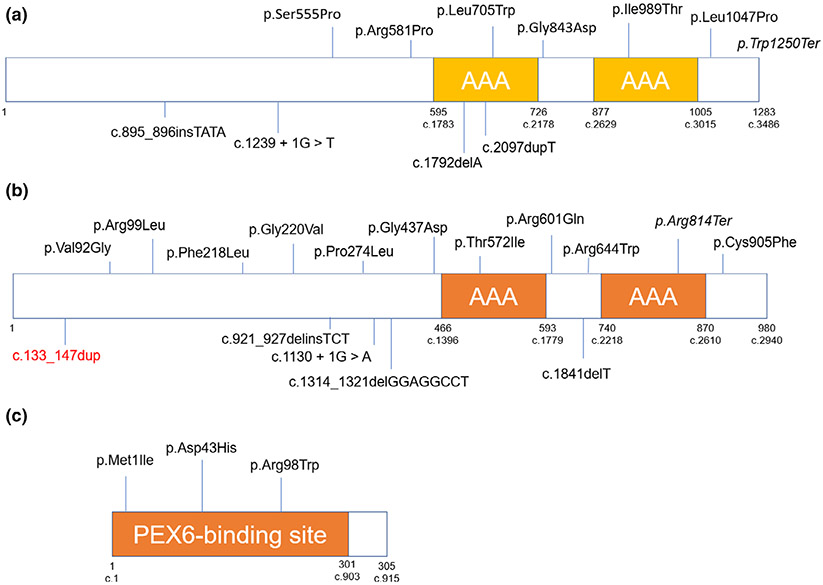
The spectrum of peroxisomal disorders is wide and comprises individuals that die in the first year of life, as well as people with sensorineural hearing loss, retinal dystrophy and amelogenesis imperfecta. In this article, we describe three patients; two diagnosed with Heimler syndrome and a third one with a mild-intermediate phenotype. We arrived at these diagnoses by conducting complete ophthalmic (National Eye Institute), auditory (National Institute of Deafness and Other Communication Disorders), and dental (National Institute of Dental and Craniofacial Research) evaluations, as well as laboratory and genetic testing. Retinal degeneration with macular cystic changes, amelogenesis imperfecta, and sensorineural hearing loss were features shared by the three patients. Patients A and C had pathogenic variants in PEX1 and Patient B, in PEX6. Besides analyzing these cases, we review the literature regarding mild peroxisomal disorders, their pathophysiology, genetics, differential diagnosis, diagnostic methods, and management. We suggest that peroxisomal disorders are considered in every child with sensorineural hearing loss and retinal degeneration. These patients should have a dental evaluation to rule out amelogenesis imperfecta as well as audiologic examination and laboratory testing including peroxisomal biomarkers and genetic testing. Appropriate diagnosis can lead to better genetic counseling and management of the associated comorbidities.
Keywords: amelogenesis imperfect; heimler syndrome; peroxisomal disorders; retinal degeneration; sensorineural hearing loss.
Published [2020]. This article is a U.S. Government work and is in the public domain in the USA.
Figures
Similar articles
-
Heimler Syndrome.Adv Exp Med Biol. 2020;1299:81-87. doi: 10.1007/978-3-030-60204-8_7. Adv Exp Med Biol. 2020. PMID: 33417209 Review.
-
Two siblings with Heimler syndrome caused by PEX1 variants: follow-up of ophthalmologic findings.Ophthalmic Genet. 2021 Aug;42(4):480-485. doi: 10.1080/13816810.2021.1923033. Epub 2021 May 6. Ophthalmic Genet. 2021. PMID: 33955814
-
Ophthalmic Manifestations of Heimler Syndrome in Two Siblings With PEX1 Variants.J Pediatr Ophthalmol Strabismus. 2024 Jan-Feb;61(1):59-66. doi: 10.3928/01913913-20230220-01. Epub 2023 Apr 24. J Pediatr Ophthalmol Strabismus. 2024. PMID: 37092661 Review.
-
Severe early onset retinitis pigmentosa in a Moroccan patient with Heimler syndrome due to novel homozygous mutation of PEX1 gene.Eur J Med Genet. 2016 Oct;59(10):507-11. doi: 10.1016/j.ejmg.2016.09.004. Epub 2016 Sep 12. Eur J Med Genet. 2016. PMID: 27633571
-
Ophthalmic manifestations of Heimler syndrome due to PEX6 mutations.Ophthalmic Genet. 2018 Jun;39(3):384-390. doi: 10.1080/13816810.2018.1432063. Ophthalmic Genet. 2018. PMID: 29676688
Cited by
-
PEX6 Mutations in Peroxisomal Biogenesis Disorders: An Usher Syndrome Mimic.Ophthalmol Sci. 2021 May 25;1(2):100028. doi: 10.1016/j.xops.2021.100028. eCollection 2021 Jun. Ophthalmol Sci. 2021. PMID: 36249295 Free PMC article.
-
Peroxisomal Disorders and Their Mouse Models Point to Essential Roles of Peroxisomes for Retinal Integrity.Int J Mol Sci. 2021 Apr 15;22(8):4101. doi: 10.3390/ijms22084101. Int J Mol Sci. 2021. PMID: 33921065 Free PMC article. Review.
-
Ocular Manifestations in Patients with Sensorineural Hearing Loss.J Ophthalmic Vis Res. 2022 Nov 29;17(4):551-573. doi: 10.18502/jovr.v17i4.12321. eCollection 2022 Oct-Dec. J Ophthalmic Vis Res. 2022. PMID: 36620710 Free PMC article. Review.
-
Introduction to the special issue on Ophthalmic Genetics: Vision in 2020.Am J Med Genet C Semin Med Genet. 2020 Sep;184(3):535-537. doi: 10.1002/ajmg.c.31841. Epub 2020 Aug 31. Am J Med Genet C Semin Med Genet. 2020. PMID: 32864823 Free PMC article.
-
Management of oral manifestations of a child with Heimler Syndrome-2.BMJ Case Rep. 2024 Apr 24;17(4):e257354. doi: 10.1136/bcr-2023-257354. BMJ Case Rep. 2024. PMID: 38663901
References
-
- Braverman N, Argyriou C, & Moser A (2014). Human disorders of peroxisome biogenesis: Zellweger spectrum and rhizomelic chondrodysplasia punctata. In Molecular machines involved in peroxisome biogenesis and maintenance (pp. 63–90). Vienna, Austria: Springer.
-
- Braverman NE, Raymond GV, Rizzo WB, Moser AB, Wilkinson ME, Stone EM, … Bose M (2016). Peroxisome biogenesis disorders in the Zellweger spectrum: An overview of current diagnosis, clinical manifestations, and treatment guidelines. Molecular Genetics and Metabolism, 117(3), 313–321. 10.1016/j.ymgme.2015.12.009 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
