

Artifacts in Musculoskeletal Ultrasonography: From Physics to Clinics
- PMID: 32867385
- PMCID: PMC7555047
- DOI: 10.3390/diagnostics10090645
Artifacts in Musculoskeletal Ultrasonography: From Physics to Clinics
Abstract
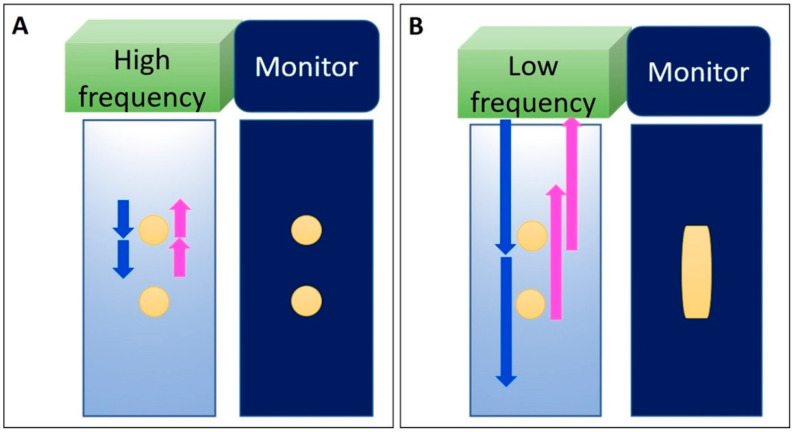
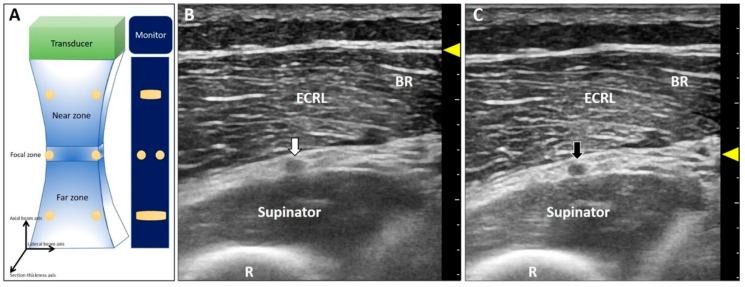
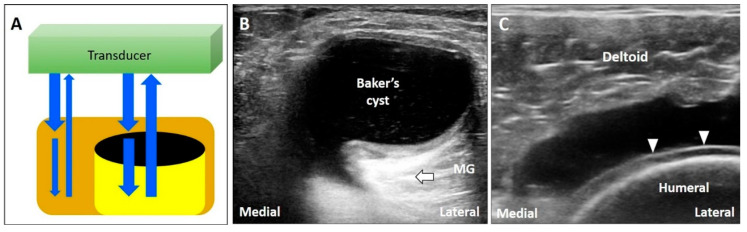
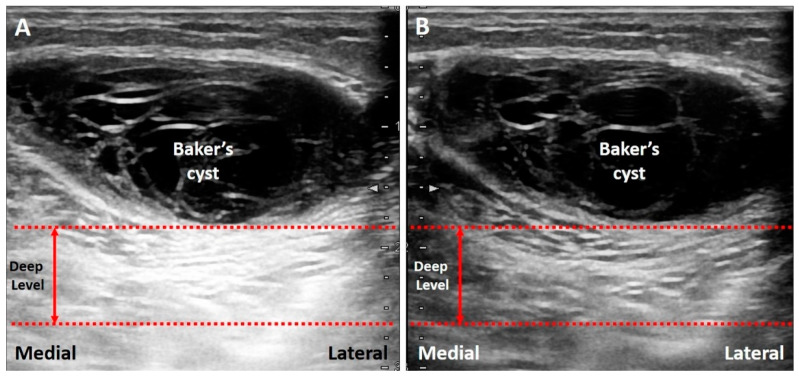
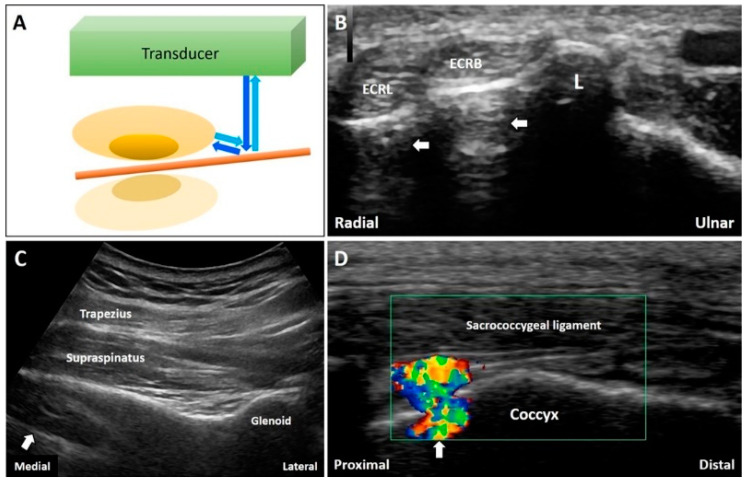
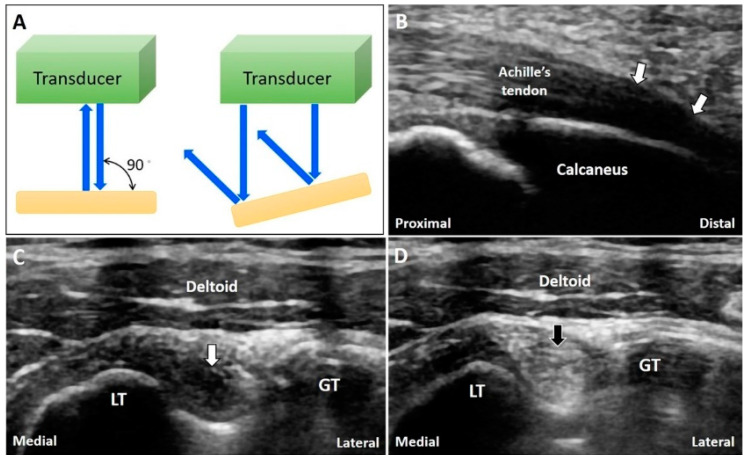
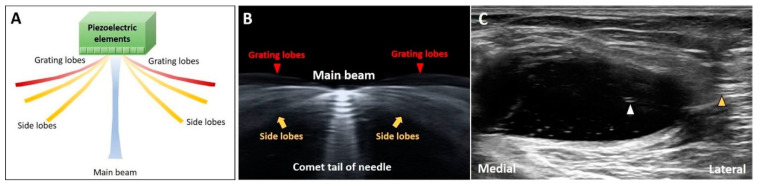
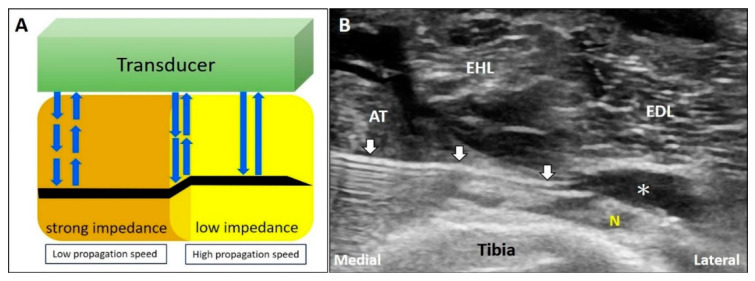
Ultrasound appears to be the most useful imaging tool in the diagnosis and guided treatment of musculoskeletal disorders. However, ultrasonography has been criticized for being user dependent. Therefore, medical professionals should be familiar with the basic principles of ultrasound imaging (e.g., physics and technical skills) to diminish artifacts and avoid misinterpretation. In this review, we focused on the physics of common artifacts, their clinical significance, and the ways to tackle them in daily practice during musculoskeletal imaging. In particular, artifacts pertaining to the focal zone, beam attenuation, path and side lobe of the beam, speed of the sound, and range ambiguity were described.
Keywords: artifact; attenuation; beam; musculoskeletal; reflection; ultrasound.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Clinical Significance of US Artifacts.Radiographics. 2017 Sep-Oct;37(5):1408-1423. doi: 10.1148/rg.2017160175. Epub 2017 Aug 4. Radiographics. 2017. PMID: 28777700 Review.
-
Artifacts in ultrasound imaging.J Ultrasound Med. 1986 Apr;5(4):227-37. doi: 10.7863/jum.1986.5.4.227. J Ultrasound Med. 1986. PMID: 3514956 Review.
-
[Ultrasonic imaging artifacts. Physical bases].Radiologe. 1993 Jan;33(1):1-10. Radiologe. 1993. PMID: 8441800 Review. German.
-
Review of artifacts associated with transrectal ultrasound: understanding, recognition, and prevention of misinterpretation.J Clin Ultrasound. 1995 Oct;23(8):483-94. doi: 10.1002/jcu.1870230805. J Clin Ultrasound. 1995. PMID: 7499519 Review.
-
Contrast-Enhanced Sonography of the Liver: How to Avoid Artifacts.Diagnostics (Basel). 2024 Aug 20;14(16):1817. doi: 10.3390/diagnostics14161817. Diagnostics (Basel). 2024. PMID: 39202305 Free PMC article. Review.
Cited by
-
Diagnostic Musculoskeletal Ultrasound for Medial Collateral Ligament Injuries: Applications in Rehabilitation.Int J Sports Phys Ther. 2024 Sep 1;19(9):1166-1171. doi: 10.26603/001c.122931. eCollection 2024. Int J Sports Phys Ther. 2024. PMID: 39246412 Free PMC article.
-
Ultrasound Imaging and Guidance for Cervical Myofascial Pain: A Narrative Review.Int J Environ Res Public Health. 2023 Feb 21;20(5):3838. doi: 10.3390/ijerph20053838. Int J Environ Res Public Health. 2023. PMID: 36900848 Free PMC article. Review.
-
Ultrasound imaging of the axilla.Insights Imaging. 2023 May 11;14(1):78. doi: 10.1186/s13244-023-01430-9. Insights Imaging. 2023. PMID: 37166516 Free PMC article. Review.
-
The (ProteUS) Anisotropy Effect in Deep Fascia Ultrasonography: The Impact of Probe Angulation on Echogenicity and Thickness Assessments.Life (Basel). 2025 May 21;15(5):822. doi: 10.3390/life15050822. Life (Basel). 2025. PMID: 40430248 Free PMC article.
-
Common and Uncommon Errors in Emergency Ultrasound.Diagnostics (Basel). 2022 Mar 4;12(3):631. doi: 10.3390/diagnostics12030631. Diagnostics (Basel). 2022. PMID: 35328184 Free PMC article. Review.
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
