

Clinical and imaging profiles of pulmonary embolism: a single-institution experience
- PMID: 32867676
- PMCID: PMC7457516
- DOI: 10.1186/s12245-020-00303-y
Clinical and imaging profiles of pulmonary embolism: a single-institution experience
Abstract
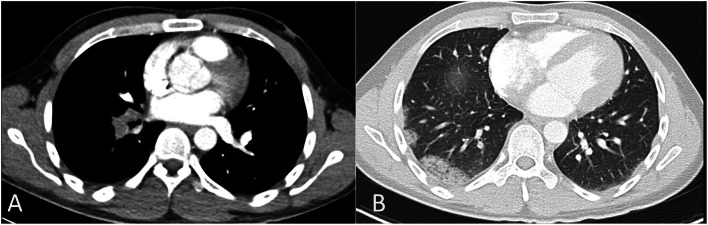
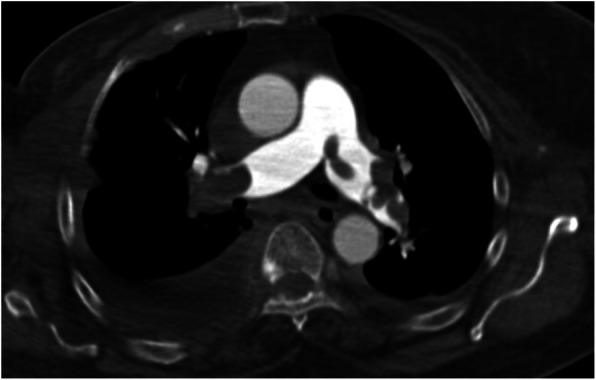
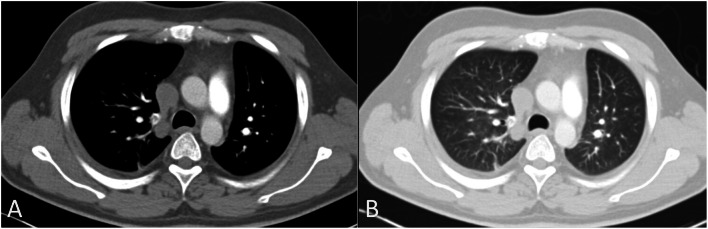
Background: Pulmonary embolism (PE) is a common life-threatening condition with non-specific clinical presentations. The diagnosis of PE depends highly on imaging studies, which may also provide prognostic information. This study aimed to describe the clinical and imaging profiles of patients with PE, emphasizing the differences between central and peripheral PE.
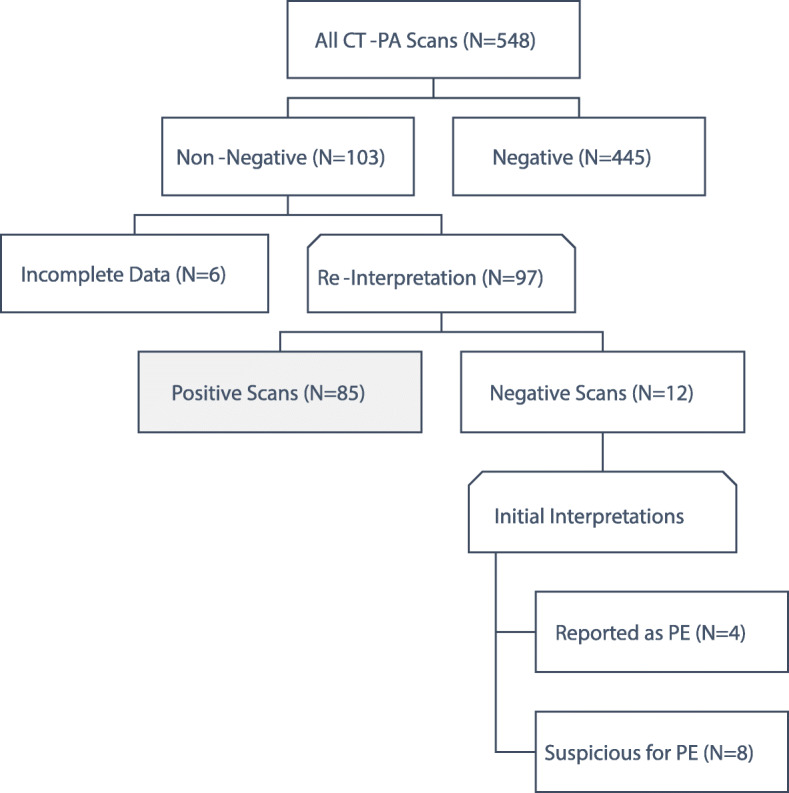
Methods: After ethics review board approval, this retrospective observational study examined the non-negative results in adult patients who underwent computed tomography pulmonary angiography (CT-PA) at our hospital between May 2016 and December 2019. Demographic and clinical information and imaging findings were collected from the electronic medical records.
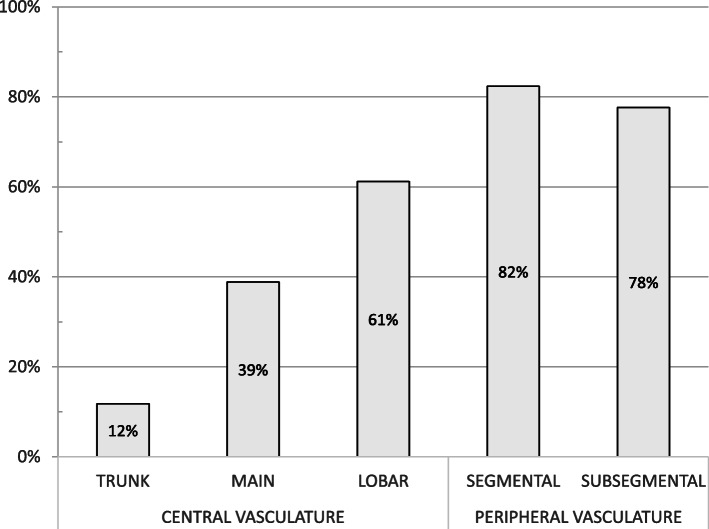
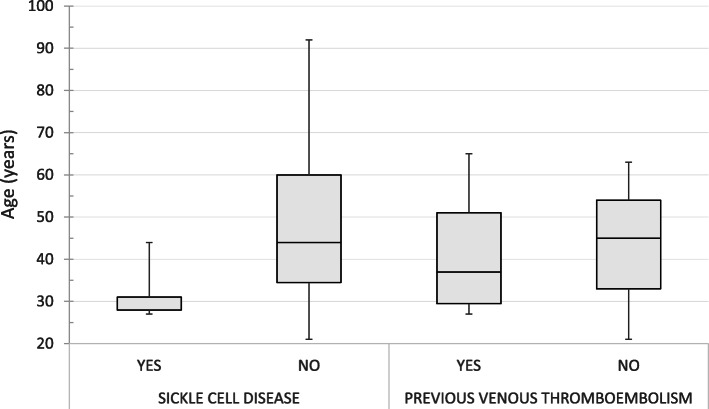
Results: The study included 85 cases that were identified after re-interpreting the 103 non-negative CT-PA scans. Six cases were excluded for incomplete data and 12 cases were false-positive. Central PE was found in 63.5% of the cases. Obesity was the most common risk factor seen in 37.6% of the cases. Furthermore, 9.4% of the patients had sickle cell disease, which tended to be associated with peripheral PE. There was no difference between the peripheral and central PE in most clinical and imaging parameters evaluated (P > 0.05). However, patients with isolated subsegmental PE were more likely to develop hemoptysis (P = 0.04).
Conclusion: This study suggests that patients with obesity and sickle cell disease constitute an important proportion of all PE cases. Furthermore, the clinical and imaging profiles in patients with peripheral PE are similar to those in patients with central PE. Future research should focus on the clinical value of peripheral PE in patients with sickle cell disease.
Keywords: Computed tomography angiography; Obesity; Pulmonary embolism; Sickle cell disease.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Karabulut N, Kiroglu Y. Relationship of parenchymal and pleural abnormalities with acute pulmonary embolism: CT findings in patients with and without embolism. Diagn Interv Radiol. 2008;14(4):189. - PubMed
LinkOut - more resources
Full Text Sources
