

Exploring trends in admissions and treatment for ankle fractures: a longitudinal cohort study of routinely collected hospital data in England
- PMID: 32867779
- PMCID: PMC7457765
- DOI: 10.1186/s12913-020-05682-9
Exploring trends in admissions and treatment for ankle fractures: a longitudinal cohort study of routinely collected hospital data in England
Abstract
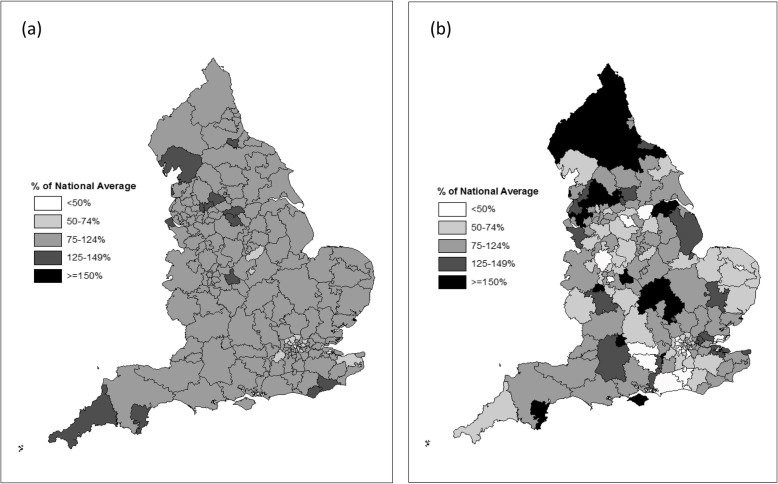
Background: Evidence on the most effective and cost-effective management of ankle fractures is sparse but evolving. A recent large RCT in older patients with unstable fractures found that management with close-contact-casting was functionally equivalent and more cost-effective than internal fixation. We describe temporal and geographic variation in ankle fracture management and estimate the potential savings if close-contact-casting was used more often in older patients.
Methods: Patients admitted to hospital in England between 2007/08 and 2016/17 with an ankle fracture were identified using routine hospital episode statistics. We tested whether the use of internal fixation, and the proportion of internal fixations using intramedullary implants, changed over time. We estimated the potential annual cost savings if patients aged 60+ years were treated with close-contact-casting rather than internal fixation, in line with emerging evidence.
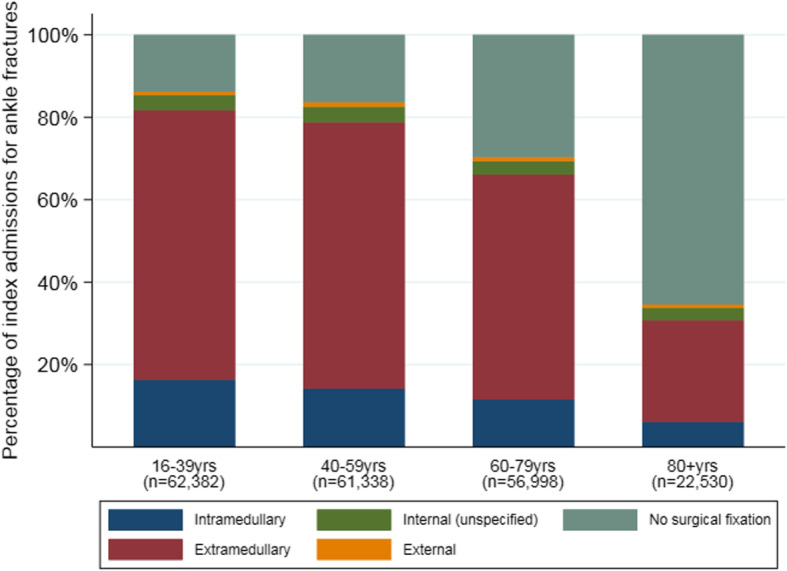
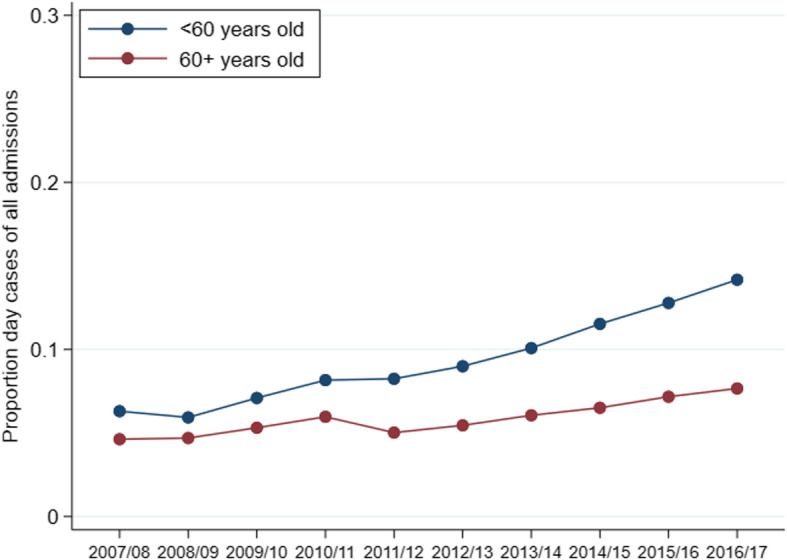
Results: Over the 10-year period, there were 223,465 hospital admissions with a primary ankle fracture diagnosis. The incidence (per 100,000) of internal fixation was fairly consistent over time in younger (33.2 in 2007/08, 30.9 in 2016/17) and older (36.5 in 2007/08, 37.4 in 2016/17) patients. The proportion of internal fixations which used intramedullary implants increased in both age groups (17.0-19.5% < 60 years; 15.2-17.4% 60+ years). In 2016/17, the cost of inpatient hospital care for ankle fractures in England was over £63.1million. If 50% of older patients who had an internal fixation instead had close-contact-casting, we estimate that approximately £1.56million could have been saved.
Conclusions: Despite emerging evidence that non-surgical and surgical management achieve equivalent functional outcomes in older patients, the rate of surgical fixation has remained relatively stable over the decade. The health service could achieve substantial savings if a higher proportion of older patients were treated with close-contact-casting, in line with recent evidence.
Keywords: Ankle fracture; Close-contact-casting; England; Extramedullary fixation; Hospital admission; Intramedullary fixation.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- Bielska IA, Wang X, Lee R, et al. The health economics of ankle and foot sprains and fractures: A systematic review of English-language published papers. Part 2: The direct and indirect costs of injury. Foot (Edinb). 2019;39:115–21. - PubMed
-
- Donken CC, Al-Khateeb H, Verhofstad MH, et al. Surgical versus conservative interventions for treating ankle fractures in adults. Cochrane Database Syst Rev. 2012;8:CD008470. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
