

Wrist movements induce torque and lever force in the scaphoid: an ex vivo study
- PMID: 32867789
- PMCID: PMC7457810
- DOI: 10.1186/s13018-020-01897-y
Wrist movements induce torque and lever force in the scaphoid: an ex vivo study
Abstract
Purpose: We hypothesised that intercarpal K-wire fixation of adjacent carpal bones would reduce torque and lever force within a fractured scaphoid bone.
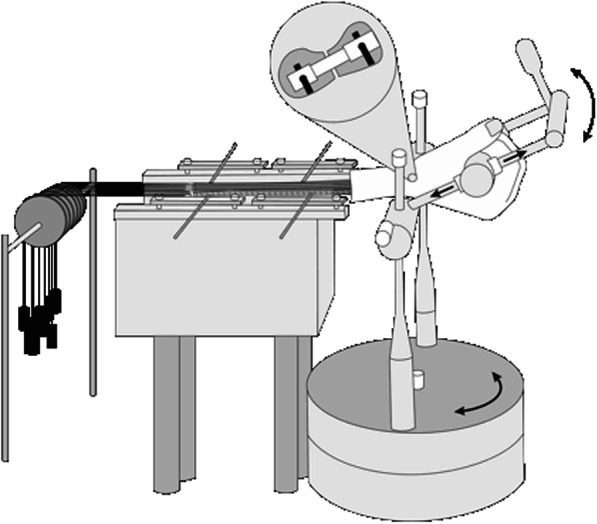
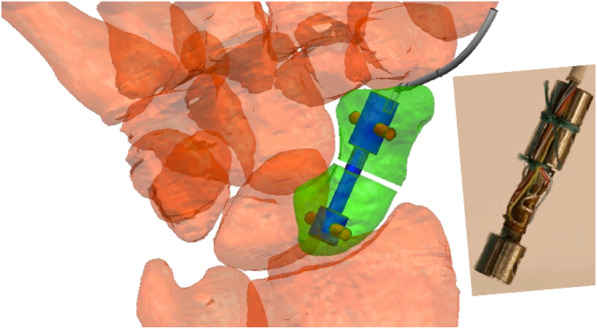
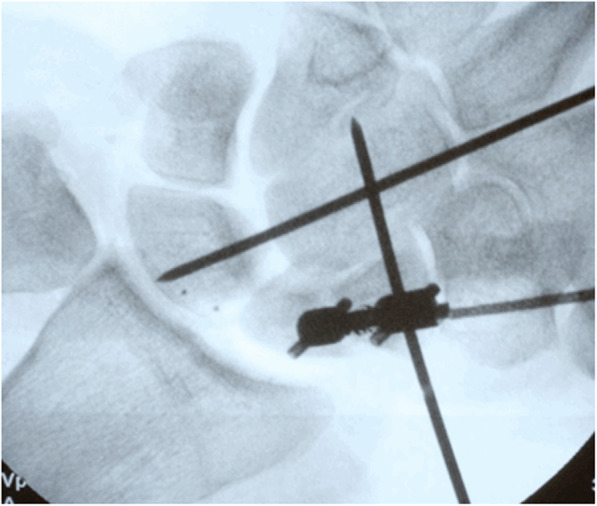
Methods: In eight cadaver wrists, a scaphoid osteotomy was stabilised using a locking nail, which also functioned as a sensor to measure isometric torque and lever forces between the fragments. The wrist was moved through 80% of full range of motion (ROM) to generate torque and force within the scaphoid. Testing was performed with and without loading of the wrist and K-wire stabilisation of the adjacent carpal bones.
Results: Average torque and lever force values were 49.6 ± 25.1 Nmm and 3.5 ± 0.9 N during extension and 41 ± 26.7 Nmm and 8.1 ± 2.8 N during flexion. Torque and lever force did not depend on scaphoid size, individual wrist ROM, or deviations of the sensor versus the anatomic axis. K-wire fixation did not produce significant changes in average torque and lever force values except with wrist radial abduction (P = 0.0485). Other than wrist extension, torque direction was not predictable.
Conclusion: In unstable scaphoid fractures, we suggest securing rotational stability with selected implants for functional postoperative care. Wrist ROM within 20% extension and radial abduction to 50% flexion limit torque and lever force exacerbation between scaphoid fragments.
Keywords: Biomechanics; Scaphoid fracture; Torque and lever force; Wrist movement.
Conflict of interest statement
The authors declare no competing financial and non-financial interests.
Figures


Similar articles
-
Screw fixation of scaphoid fractures: a biomechanical assessment of screw length and screw augmentation.J Hand Surg Am. 2006 Mar;31(3):405-13. doi: 10.1016/j.jhsa.2005.09.014. J Hand Surg Am. 2006. PMID: 16516734
-
Scaphoid interfragmentary motions due to simulated transverse fracture and volar wedge osteotomy.Clin Biomech (Bristol). 2014 Feb;29(2):189-95. doi: 10.1016/j.clinbiomech.2013.11.013. Epub 2013 Nov 26. Clin Biomech (Bristol). 2014. PMID: 24331861
-
[Development and biomechanical study of Ni-Ti shape memory alloys scaphoid arc nail].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2008 Jan;22(1):48-52. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2008. PMID: 18361237 Chinese.
-
Operative Treatment of Acute Scaphoid Fractures.Hand Surg. 2015;20(2):210-4. doi: 10.1142/S021881041540002X. Hand Surg. 2015. PMID: 26051762 Review.
-
Surgical Strategy for Scaphoid Nonunion Treatment.J Hand Surg Asian Pac Vol. 2018 Dec;23(4):450-462. doi: 10.1142/S2424835518300049. J Hand Surg Asian Pac Vol. 2018. PMID: 30428803 Review.
Cited by
-
Sex-Specific Size Analysis of Carpal Bones: Implications for Orthopedic Biomedical Device Design and Therapy Planning.Life (Basel). 2024 Jan 18;14(1):140. doi: 10.3390/life14010140. Life (Basel). 2024. PMID: 38255755 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
