

Reducing unnecessary caesarean sections: scoping review of financial and regulatory interventions
- PMID: 32867791
- PMCID: PMC7457477
- DOI: 10.1186/s12978-020-00983-y
Reducing unnecessary caesarean sections: scoping review of financial and regulatory interventions
Abstract
Background: Caesarean sections (CS) are increasing worldwide. Financial incentives and related regulatory and legislative factors are important determinants of CS rates. This scoping review examines the evidence base of financial, regulatory and legislative interventions intended to reduce CS rates.
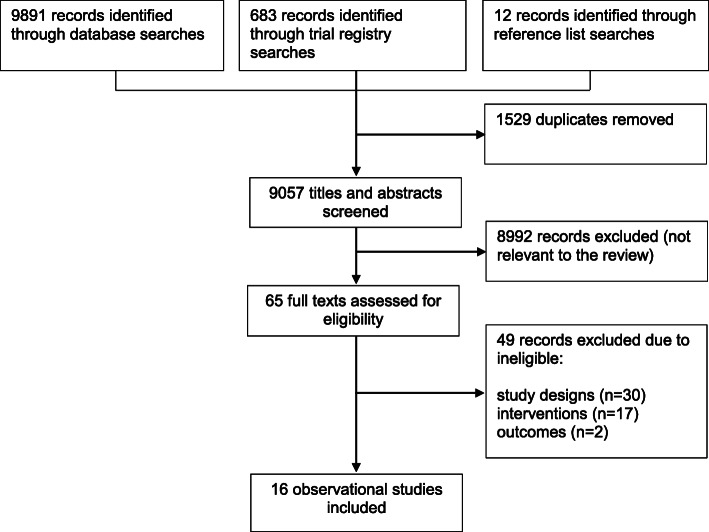
Methods: We searched MEDLINE, EMBASE, CINAHL and two trials registers in June 2019. Both experimental and observational intervention studies were eligible for inclusion. Primary outcome measures were: CS, spontaneous vaginal and instrumental birth rates. We assessed quality of evidence using Grading of Recommendations, Assessment, Development and Evaluation (GRADE) method.
Results: We identified 9057 articles and assessed 65 full-texts. We included 16 observational studies. Most of the studies were conducted in high-income countries. Three studies assessed payment methods for health workers: equalising physician fees for vaginal and caesarean delivery reduced CS rates in one study; however, little or no difference in CS rates was found in the remaining two studies. Nine studies assessed payment methods for health organisations: There was no difference in CS rates between diagnosis-related group (DRG) payment system compared to fee-for-service system in one study. However, DRG system was associated with lower odds for CS in another study. There was little or no difference in CS rates following implementation of global budget payment (GBP) system in two studies. Vaginal birth after caesarean section (VBAC) increased after implementation of a case-based payment system in one study. Caesarean section increased while VBAC rates decreased following implementation of a cap-based payment system in another study. Financial incentive for providers to promote vaginal delivery combined with free vaginal delivery policy was found to reduce CS rates in one study. Studied regulatory and legislative interventions (comprising legislatively imposed practice guidelines for physicians in one study and multi-faceted strategy which included policies to control CS on maternal request in another study) were found to reduce CS rates. The GRADE quality of evidence varied from very low to low.
Conclusions: Available evidence on the effects of financial and regulatory strategies intended to reduce unnecessary CS is inconclusive given inconsistency in effects and low quality of the available evidence. More rigorous studies are needed.
Keywords: Caesarean section; Financial interventions; Legislative interventions; Overuse; Payment mechanisms; Regulatory interventions; Scoping review.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Betrán AP, Merialdi M, Lauer JA, Bing-shun W, Thomas J, et al. Rates of caesarean section: analysis of global, regional and national estimates. Paediatr Perinat Epidemiol. 2007;21(2):98–113. - PubMed
-
- Boerma T, Ronsmans C, Melesse DY, Barros AJD, Barros FC, Juan L, Ann-Beth Moller AB, et al. Global epidemiology of use of and disparities in caesarean sections. Lancet. 2018;392:1341–1348. - PubMed
-
- Lumbiganon P, Laopaiboon M, Gülmezoglu AM, Souza JP, Taneepanichskul S, Ruyan P, et al. Method of delivery and pregnancy outcomes in Asia: the WHO global survey on maternal and perinatal health 2007-08. Lancet. 2010;375(9713):490–499. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
