

Cardiac changes in pediatric cancer survivors
- PMID: 32868378
- PMCID: PMC8578014
- DOI: 10.1136/jim-2020-001373
Cardiac changes in pediatric cancer survivors
Abstract
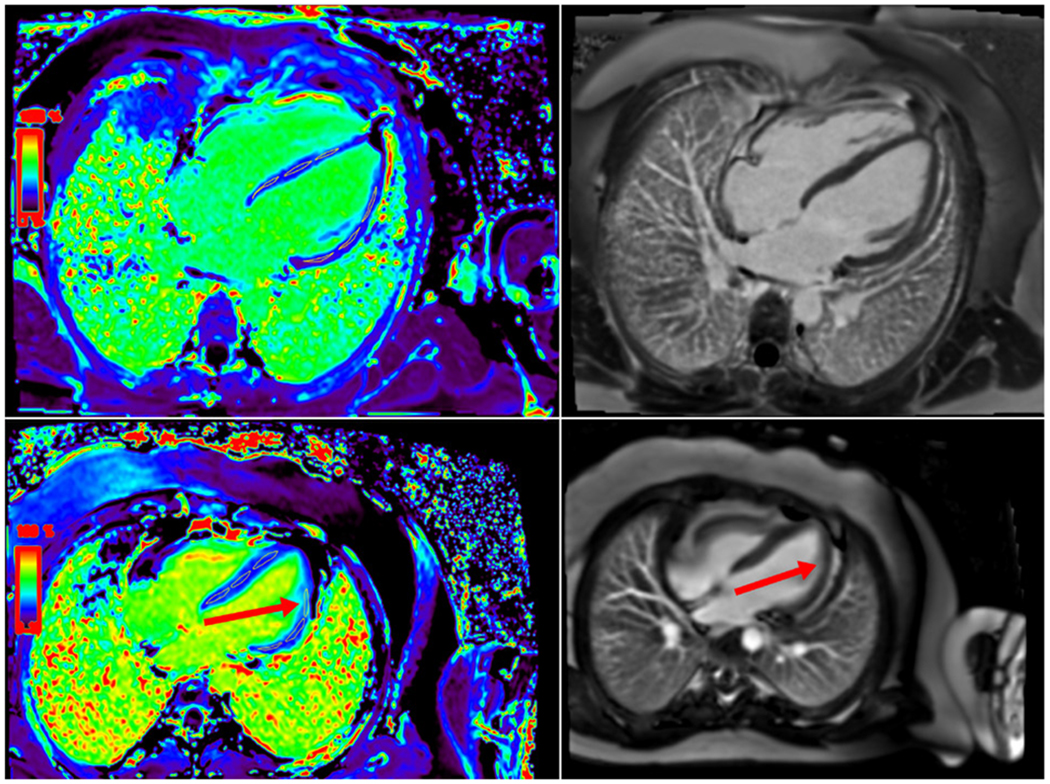
Cardiac damage from chemotherapy is a known phenomenon leading to significant morbidity and mortality in the cancer surviving population, and identifying high-risk pediatric patients early is challenging. The purpose of this pilot study was to evaluate whether echo strain, cardiac MRI (CMR), and serum biomarkers are more sensitive methods for detecting cardiac toxicity than standard echo and to examine the relationship between biomarkers in patients without decreased systolic function as determined by standard echo. In this pilot study, we prospectively enrolled pediatric subjects after completion of anthracycline inclusive chemotherapy. Each subject underwent a post-treatment echocardiogram (standard with strain), serum biomarkers (N-terminal brain natriuretic peptide (NT-pro-BNP) and interleukin 1 receptor-like 1 protein (ST2)), and CMR (standard and extracellular volumes (ECVs)). We correlated the markers using Pearson correlation. We enrolled 30 subjects, 11F/19M, aged 8-21 years. Cumulative anthracycline dose (CAD) correlated with BNP (p=0.06), CMR ECV 4-chamber (p=0.05) and sagittal (p=0.01), and mitral valve E/A (p=0.02). BNP correlated with CMR ECV 4-chamber (p=0.001) and sagittal (p=0.001) and with echo average longitudinal strain (ALS) (p=0.05). This study demonstrated a significant correlation of CAD with BNP and CMR ECV. There was also a significant correlation of NT-pro-BNP with CMR ECV and ALS. Combining these parameters with standard echo has the potential to identify high-risk patients early. Further studies are needed for long-term follow-up and management in this vulnerable population.
Keywords: biomarkers; cardiomyopathies; drug-related side effects and adverse reactions; echocardiography; leukemia.
© American Federation for Medical Research 2020. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Lipshultz SE, Adams MJ, Colan SD, et al. Long-term cardiovascular toxicity in children, adolescents, and young adults who receive cancer therapy: pathophysiology, course, monitoring, management, prevention, and research directions: a scientific statement from the American Heart Association. Circulation 2013;128:1927–95. - PubMed
-
- Kremer LCM, van Dalen EC, Offringa M, et al. Frequency and risk factors of anthracycline-induced clinical heart failure in children: a systematic review. Ann Oncol 2002;13:503–12. - PubMed
-
- Kremer LCM, van der Pal HJH, Offringa M, et al. Frequency and risk factors of subclinical cardiotoxicity after anthracycline therapy in children: a systematic review. Ann Oncol 2002;13:819–29. - PubMed
-
- Steinherz LJ, Graham T, Hurwitz R, et al. Guidelines for cardiac monitoring of children during and after anthracycline therapy: report of the Cardiology Committee of the Children’s Cancer Study Group. Pediatrics 1992;89:942–9. - PubMed
-
- Shankar SM, Marina N, Hudson MM, et al. Monitoring for cardiovascular disease in survivors of childhood cancer: report from the Cardiovascular Disease Task Force of the Children’s Oncology Group. Pediatrics 2008;121:e387–96. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
