

Subarachnoid neurocysticercosis: emerging concepts and treatment
- PMID: 32868512
- PMCID: PMC7733161
- DOI: 10.1097/QCO.0000000000000669
Subarachnoid neurocysticercosis: emerging concepts and treatment
Abstract
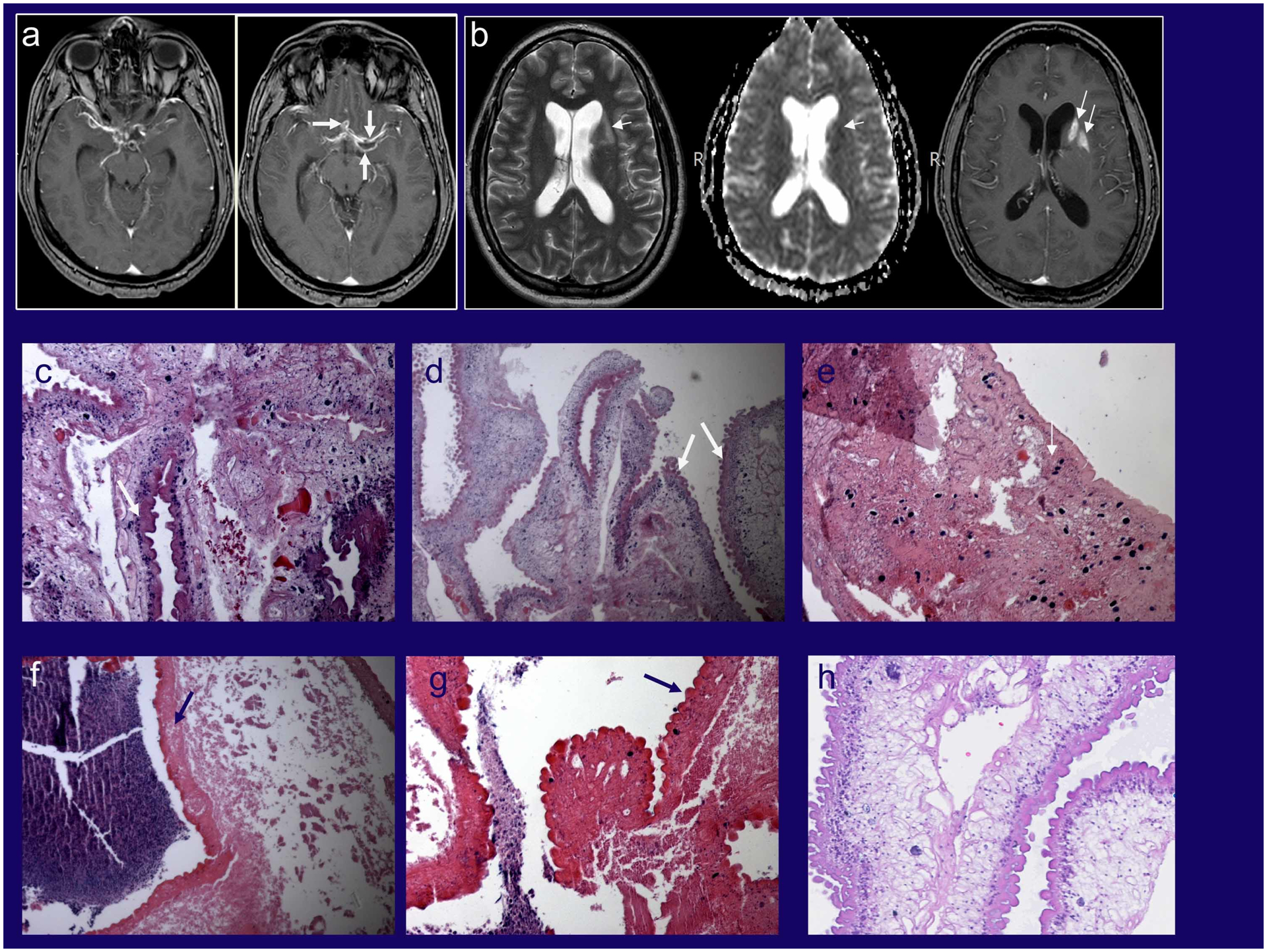
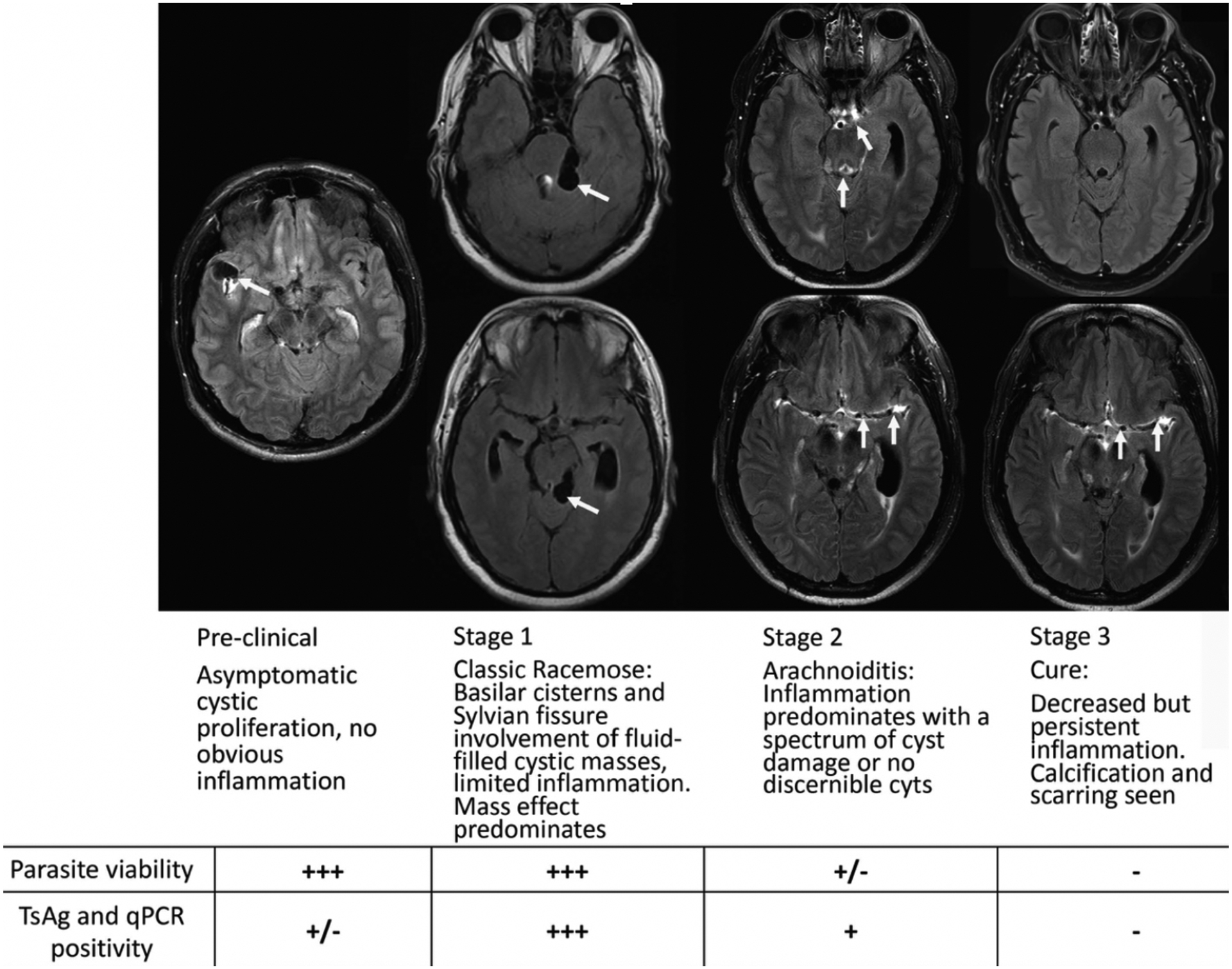
Purpose of review: Subarachnoid neurocysticercosis (SUBNCC) is caused by a morphologically unique proliferative form of Taenia solium involving the subarachnoid spaces. Prolonged therapy based upon the pathophysiology of SUBNCC and long-term follow-up have shed light on the course of disease and led to highly improved outcomes.
Recent findings: SUBNCC has a prolonged incubation period of between 10 and 25 years characterized by cyst proliferation and growth and invasion of contiguous spaces leading to mass effect (Stage 1). With induction of the host-immune responses, cysts degenerate leading to a predominately inflammatory arachnoiditis (Stage 2) causing hydrocephalus, infarcts, and other inflammatory based neurological manifestations. Inactive disease (Stage 3) may occur naturally but mostly is a result of successful treatment, which generally requires prolonged intensive anthelminthic and antiinflammatory treatments. Cerebral spinal fluid cestode antigen or cestode DNA falling to nondetectable levels predicts effective treatment. Prolonged treatment with extended follow-up has resulted in moderate disability and no mortality. Repeated short intensive 8-14-day courses of treatment are also used, but long-term outcomes and safety using this strategy are not reported.
Summary: SUBNCC gives rise to a chronic arachnoiditis. Its unique ability to proliferate and induce inflammatory responses requires long-term anthelmintic and antiinflammatory medications.
Conflict of interest statement
Figures
References
-
- Hinojosa-Juarez AC, Sandoval-Balanzario M, McManus DP, Monroy-Ostria A. Genetic similarity between cysticerci of Taenia solium isolated from human brain and from pigs. Infection Genetics and Evolution. 2008;8(5):653–6. - PubMed
-
- Rabiela MT, Rivas-Hernandez A, Rodriquez-Ibarra J, Castilo-Medina S, Cancino FdM. Anatomopathological Aspects of Human Brain Cysticercosis In: Flisser A, Willms k, Laclette JP, Larralde C, Ridaura C, Beltran F, editors. Cysticercosis: Present State of Knowledge and Prespectives. New York, New York: Academic Press; 1982. p. 179–200.
-
- Rabiela MT, Rivas A, Flisser A. Morphological types of Taenia solium cysticerci. Parasitol Today. 1989;5(11):357–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
