

Efficacy of immune-checkpoint inhibitors in metastatic gastric or gastroesophageal junction adenocarcinoma by patient subgroups: A systematic review and meta-analysis
- PMID: 32869544
- PMCID: PMC7571828
- DOI: 10.1002/cam4.3417
Efficacy of immune-checkpoint inhibitors in metastatic gastric or gastroesophageal junction adenocarcinoma by patient subgroups: A systematic review and meta-analysis
Abstract
Background: Efficacy of immune checkpoint inhibitors (ICIs) in metastatic gastric/gastroesophageal junction (GEJ) adenocarcinoma is inconsistent. Whether the efficacy of ICIs is comparable across different subgroups remains unknown.
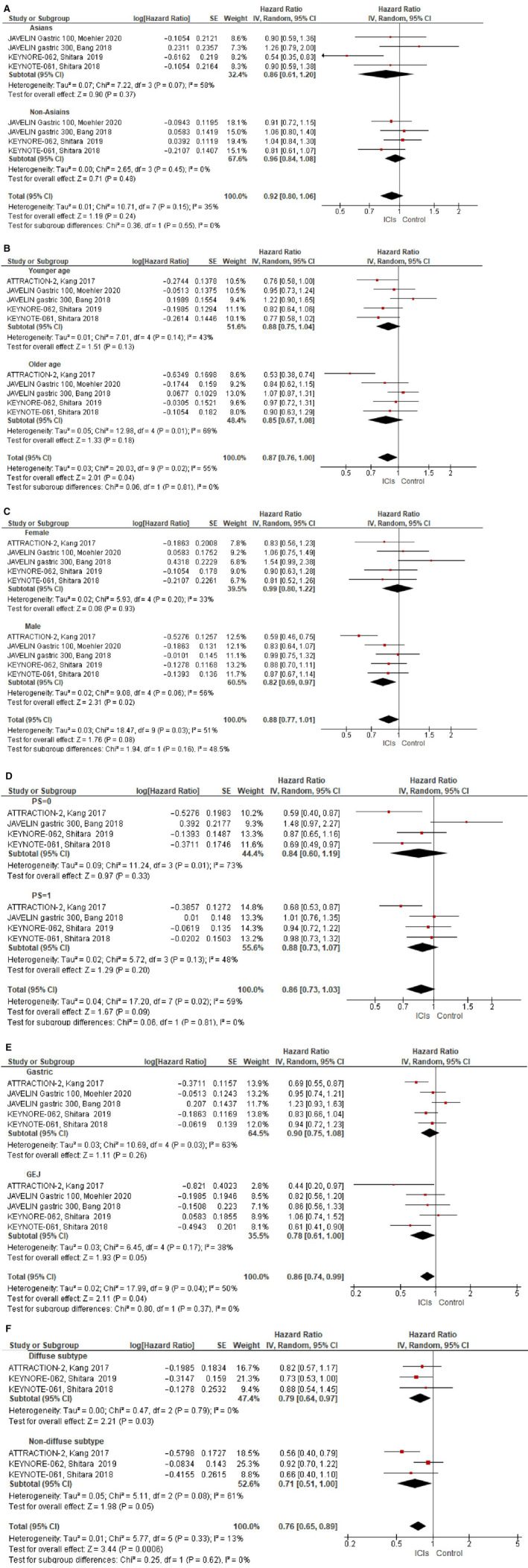
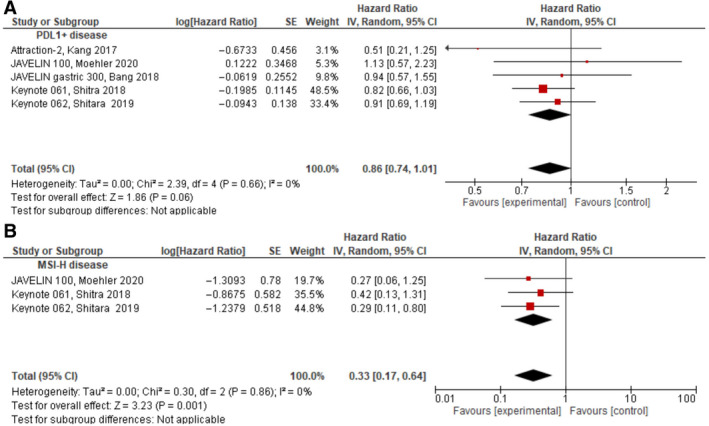
Methods: We identified randomized controlled trials (RCTs) that compared standard treatment for metastatic gastric/GEJ adenocarcinoma to ICIs. Hazard ratios (HRs) and 95% confidence intervals (CI) for overall survival (OS) were extracted and pooled in a meta-analysis. Prespecified subgroups were included as follows: age at randomization (</≤65 vs ≥/>65 years), gender (female vs male), ethnicity (Asians vs non-Asians), performance-status (0 vs 1), tumor location (gastric vs GEJ), and histological subtype (diffuse vs others). OS in patients with programmed death ligand (PD-L1) positive and with microsatellite instability-high (MSI-H) were also extracted and pooled in a meta-analysis.
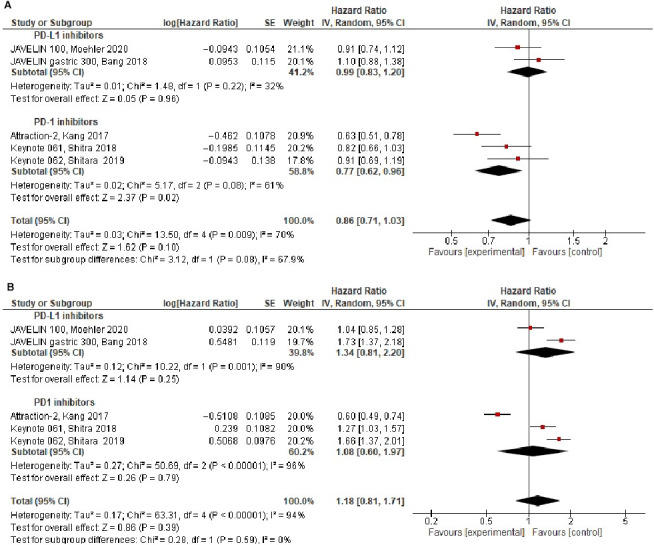
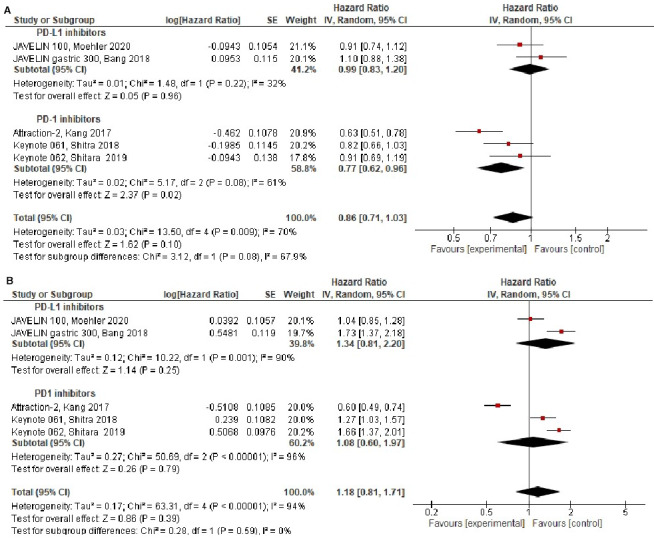
Results: Five RCTs comprising 2,264 patients were analyzed. Compared to standard therapy, ICIs did not improve OS (HR = 0.86, 95% CI 0.71-1.03, P = .10) and the effect of ICIs on OS was similar in all subgroups. Nonsignificantly greater effect sizes were seen in older patients (HR = 0.85 vs 0.88, P = .81), male (HR = 0.82 vs 0.99, P = .16), Asians (HR = 0.86 vs 0.96, P = .55), performance-status 0 (HR = 0.84 vs 0.88, P = .81), GEJ tumors (HR = 0.78 vs 0.90, P = .37), and nondiffuse subtype (HR = 0.71 vs 0.79, P = .62). ICIs were associated with significantly improved OS in patients with MSI-H (HR = 0.33, P = .001), but not in PD-L1 positive disease (HR = 0.86, P = .06).
Conclusions: Compared to standard treatment, ICIs in metastatic gastric/GEJ adenocarcinoma did not improve OS. None of the evaluated subgroups has shown increased magnitude of effect to ICIs, aside of the small group with MSI-H tumors.
Keywords: gastric cancer; gastroesophageal cancer; immune-checkpoint inhibitors; immunotherapy.
© 2020 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
Dr Moore declared
Figures
References
-
- Cunningham D, Starling N, Rao S, et al. Capecitabine and oxaliplatin for advanced esophagogastric cancer. N Engl J Med. 2008;358:36‐46. - PubMed
-
- Wagner AD, Grothe W, Haerting J, Kleber G, Grothey A, Fleig WE. Chemotherapy in advanced gastric cancer: a systematic review and meta‐analysis based on aggregate data. J Clin Oncol. 2006;24:2903‐2909. - PubMed
-
- Kang Y‐K, Kang W‐K, Shin D‐B, et al. Capecitabine/cisplatin versus 5‐fluorouracil/cisplatin as first‐line therapy in patients with advanced gastric cancer: a randomised phase III noninferiority trial. Ann Oncol. 2009;20:666‐673. - PubMed
-
- Galdy S, Cella CA, Spada F, et al. Systemic therapy beyond first line in advanced gastric cancer: An overview of the main randomized clinical trials. Crit Rev Oncol Hematol. 2016;99:1‐12. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
