

Community Outbreak Investigation of SARS-CoV-2 Transmission Among Bus Riders in Eastern China
- PMID: 32870239
- PMCID: PMC7489377
- DOI: 10.1001/jamainternmed.2020.5225
Community Outbreak Investigation of SARS-CoV-2 Transmission Among Bus Riders in Eastern China
Erratum in
-
Updated Information About Index Patient in Study of SARS-CoV-2 Transmission Among Bus Riders in Eastern China.JAMA Intern Med. 2021 May 1;181(5):727. doi: 10.1001/jamainternmed.2020.8608. JAMA Intern Med. 2021. PMID: 33492332 Free PMC article. No abstract available.
Abstract
Importance: Evidence of whether severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes coronavirus disease 2019 (COVID-19), can be transmitted as an aerosol (ie, airborne) has substantial public health implications.
Objective: To investigate potential transmission routes of SARS-CoV-2 infection with epidemiologic evidence from a COVID-19 outbreak.
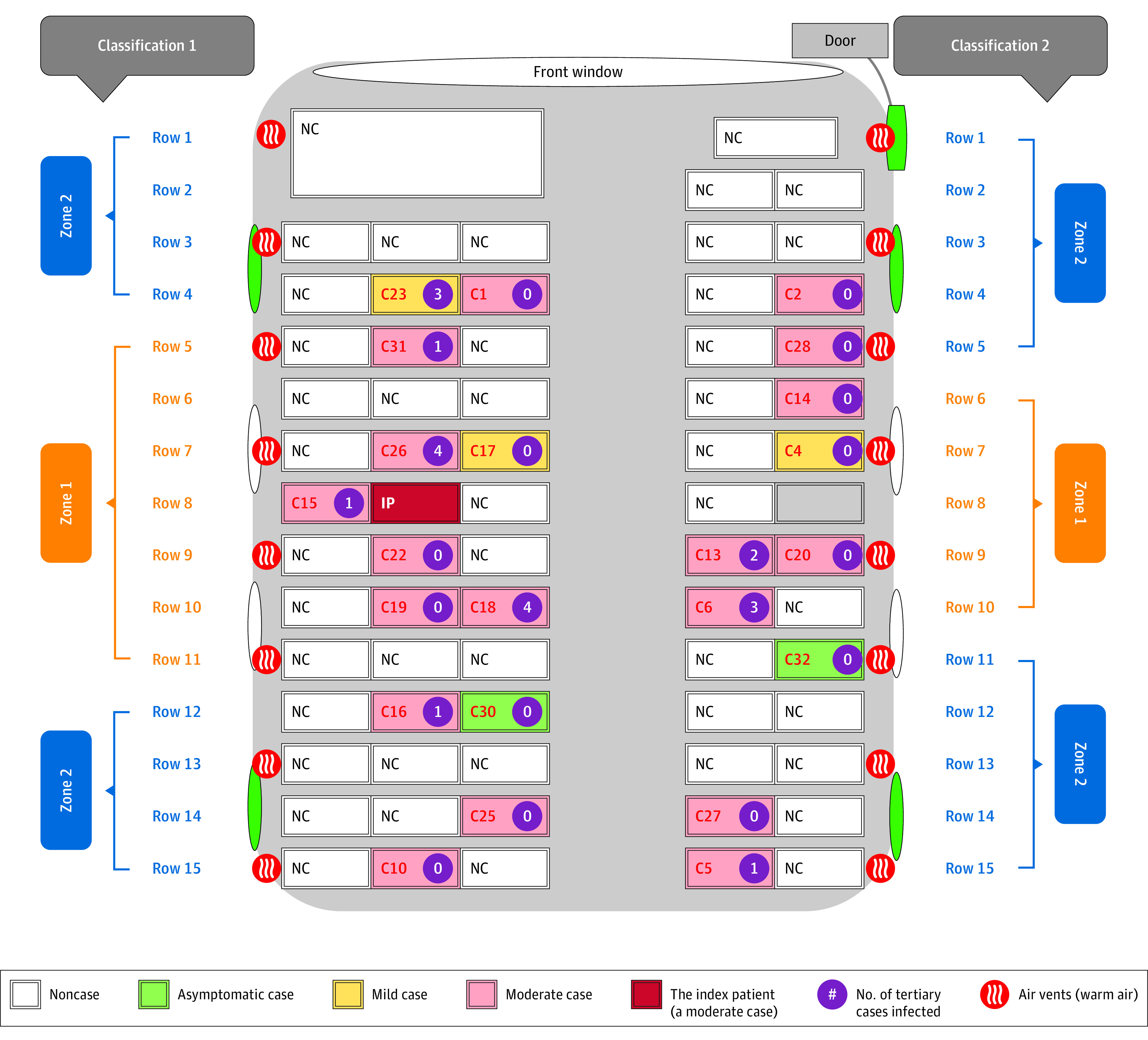
Design, setting, and participants: This cohort study examined a community COVID-19 outbreak in Zhejiang province. On January 19, 2020, 128 individuals took 2 buses (60 [46.9%] from bus 1 and 68 [53.1%] from bus 2) on a 100-minute round trip to attend a 150-minute worship event. The source patient was a passenger on bus 2. We compared risks of SARS-CoV-2 infection among at-risk individuals taking bus 1 (n = 60) and bus 2 (n = 67 [source patient excluded]) and among all other individuals (n = 172) attending the worship event. We also divided seats on the exposed bus into high-risk and low-risk zones according to the distance from the source patient and compared COVID-19 risks in each zone. In both buses, central air conditioners were in indoor recirculation mode.
Main outcomes and measures: SARS-CoV-2 infection was confirmed by reverse transcription polymerase chain reaction or by viral genome sequencing results. Attack rates for SARS-CoV-2 infection were calculated for different groups, and the spatial distribution of individuals who developed infection on bus 2 was obtained.
Results: Of the 128 participants, 15 (11.7%) were men, 113 (88.3%) were women, and the mean age was 58.6 years. On bus 2, 24 of the 68 individuals (35.3% [including the index patient]) received a diagnosis of COVID-19 after the event. Meanwhile, none of the 60 individuals in bus 1 were infected. Among the other 172 individuals at the worship event, 7 (4.1%) subsequently received a COVID-19 diagnosis. Individuals in bus 2 had a 34.3% (95% CI, 24.1%-46.3%) higher risk of getting COVID-19 compared with those in bus 1 and were 11.4 (95% CI, 5.1-25.4) times more likely to have COVID-19 compared with all other individuals attending the worship event. Within bus 2, individuals in high-risk zones had moderately, but nonsignificantly, higher risk for COVID-19 compared with those in the low-risk zones. The absence of a significantly increased risk in the part of the bus closer to the index case suggested that airborne spread of the virus may at least partially explain the markedly high attack rate observed.
Conclusions and relevance: In this cohort study and case investigation of a community outbreak of COVID-19 in Zhejiang province, individuals who rode a bus to a worship event with a patient with COVID-19 had a higher risk of SARS-CoV-2 infection than individuals who rode another bus to the same event. Airborne spread of SARS-CoV-2 seems likely to have contributed to the high attack rate in the exposed bus. Future efforts at prevention and control must consider the potential for airborne spread of the virus.
Conflict of interest statement
Figures
Comment in
-
Community Outbreak Investigation of SARS-CoV-2 Transmission Among Bus Riders in Eastern China-More Detailed Studies Are Needed.JAMA Intern Med. 2021 May 1;181(5):719-720. doi: 10.1001/jamainternmed.2020.8567. JAMA Intern Med. 2021. PMID: 33492352 No abstract available.
References
-
- World Health Organization . Coronavirus disease 2019 (COVID-19) situation report—197. Accessed August 5, 2020. https://www.who.int/docs/default-source/coronaviruse/situation-reports/2...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
