

Effect of Intraoperative Low Tidal Volume vs Conventional Tidal Volume on Postoperative Pulmonary Complications in Patients Undergoing Major Surgery: A Randomized Clinical Trial
- PMID: 32870298
- PMCID: PMC7489812
- DOI: 10.1001/jama.2020.12866
Effect of Intraoperative Low Tidal Volume vs Conventional Tidal Volume on Postoperative Pulmonary Complications in Patients Undergoing Major Surgery: A Randomized Clinical Trial
Abstract
Importance: In patients who undergo mechanical ventilation during surgery, the ideal tidal volume is unclear.
Objective: To determine whether low-tidal-volume ventilation compared with conventional ventilation during major surgery decreases postoperative pulmonary complications.
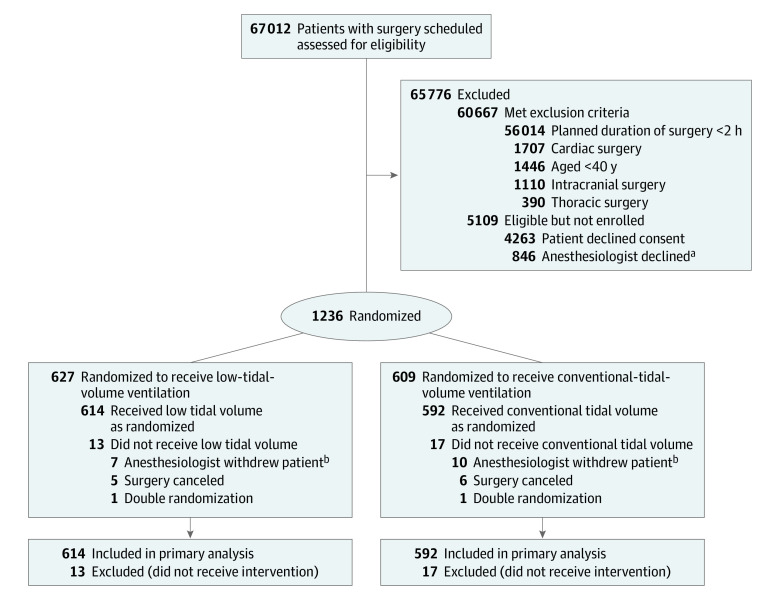
Design, setting, and participants: Single-center, assessor-blinded, randomized clinical trial of 1236 patients older than 40 years undergoing major noncardiothoracic, nonintracranial surgery under general anesthesia lasting more than 2 hours in a tertiary hospital in Melbourne, Australia, from February 2015 to February 2019. The last date of follow-up was February 17, 2019.
Interventions: Patients were randomized to receive a tidal volume of 6 mL/kg predicted body weight (n = 614; low tidal volume group) or a tidal volume of 10 mL/kg predicted body weight (n = 592; conventional tidal volume group). All patients received positive end-expiratory pressure (PEEP) at 5 cm H2O.
Main outcomes and measures: The primary outcome was a composite of postoperative pulmonary complications within the first 7 postoperative days, including pneumonia, bronchospasm, atelectasis, pulmonary congestion, respiratory failure, pleural effusion, pneumothorax, or unplanned requirement for postoperative invasive or noninvasive ventilation. Secondary outcomes were postoperative pulmonary complications including development of pulmonary embolism, acute respiratory distress syndrome, systemic inflammatory response syndrome, sepsis, acute kidney injury, wound infection (superficial and deep), rate of intraoperative need for vasopressor, incidence of unplanned intensive care unit admission, rate of need for rapid response team call, intensive care unit length of stay, hospital length of stay, and in-hospital mortality.
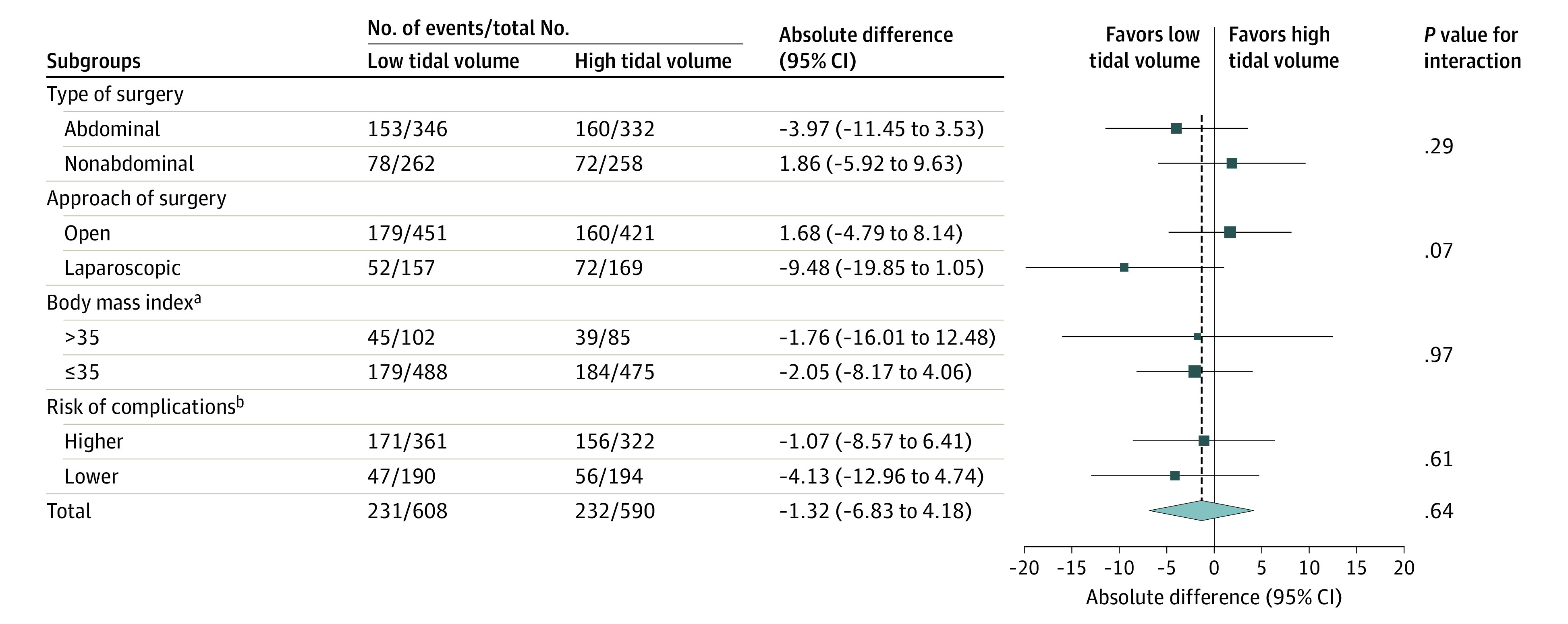
Results: Among 1236 patients who were randomized, 1206 (98.9%) completed the trial (mean age, 63.5 years; 494 [40.9%] women; 681 [56.4%] undergoing abdominal surgery). The primary outcome occurred in 231 of 608 patients (38%) in the low tidal volume group compared with 232 of 590 patients (39%) in the conventional tidal volume group (difference, -1.3% [95% CI, -6.8% to 4.2%]; risk ratio, 0.97 [95% CI, 0.84-1.11]; P = .64). There were no significant differences in any of the secondary outcomes.
Conclusions and relevance: Among adult patients undergoing major surgery, intraoperative ventilation with low tidal volume compared with conventional tidal volume, with PEEP applied equally between groups, did not significantly reduce pulmonary complications within the first 7 postoperative days.
Trial registration: ANZCTR Identifier: ACTRN12614000790640.
Conflict of interest statement
Figures
Comment in
-
Effect of Tidal Volume on Pulmonary Outcomes After Surgery.JAMA. 2021 Jan 19;325(3):306. doi: 10.1001/jama.2020.22627. JAMA. 2021. PMID: 33464328 No abstract available.
-
Effect of Tidal Volume on Pulmonary Outcomes After Surgery.JAMA. 2021 Jan 19;325(3):307. doi: 10.1001/jama.2020.22630. JAMA. 2021. PMID: 33464329 No abstract available.
-
Effect of Tidal Volume on Pulmonary Outcomes After Surgery.JAMA. 2021 Jan 19;325(3):306-307. doi: 10.1001/jama.2020.22633. JAMA. 2021. PMID: 33464330 No abstract available.
References
-
- Fernandez-Bustamante A, Frendl G, Sprung J, et al. . Postoperative pulmonary complications, early mortality, and hospital stay following noncardiothoracic surgery: a multicenter study by the Perioperative Research Network Investigators. JAMA Surg. 2017;152(2):157-166. doi:10.1001/jamasurg.2016.4065 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
