

Methods for the defining mechanisms of anterior vaginal wall descent (DEMAND) study
- PMID: 32870340
- PMCID: PMC7917148
- DOI: 10.1007/s00192-020-04511-1
Methods for the defining mechanisms of anterior vaginal wall descent (DEMAND) study
Abstract
Introduction and hypothesis: The protocol and analysis methods for the Defining Mechanisms of Anterior Vaginal Wall Descent (DEMAND) study are presented. DEMAND was designed to identify mechanisms and contributors of prolapse recurrence after two transvaginal apical suspension procedures for uterovaginal prolapse.
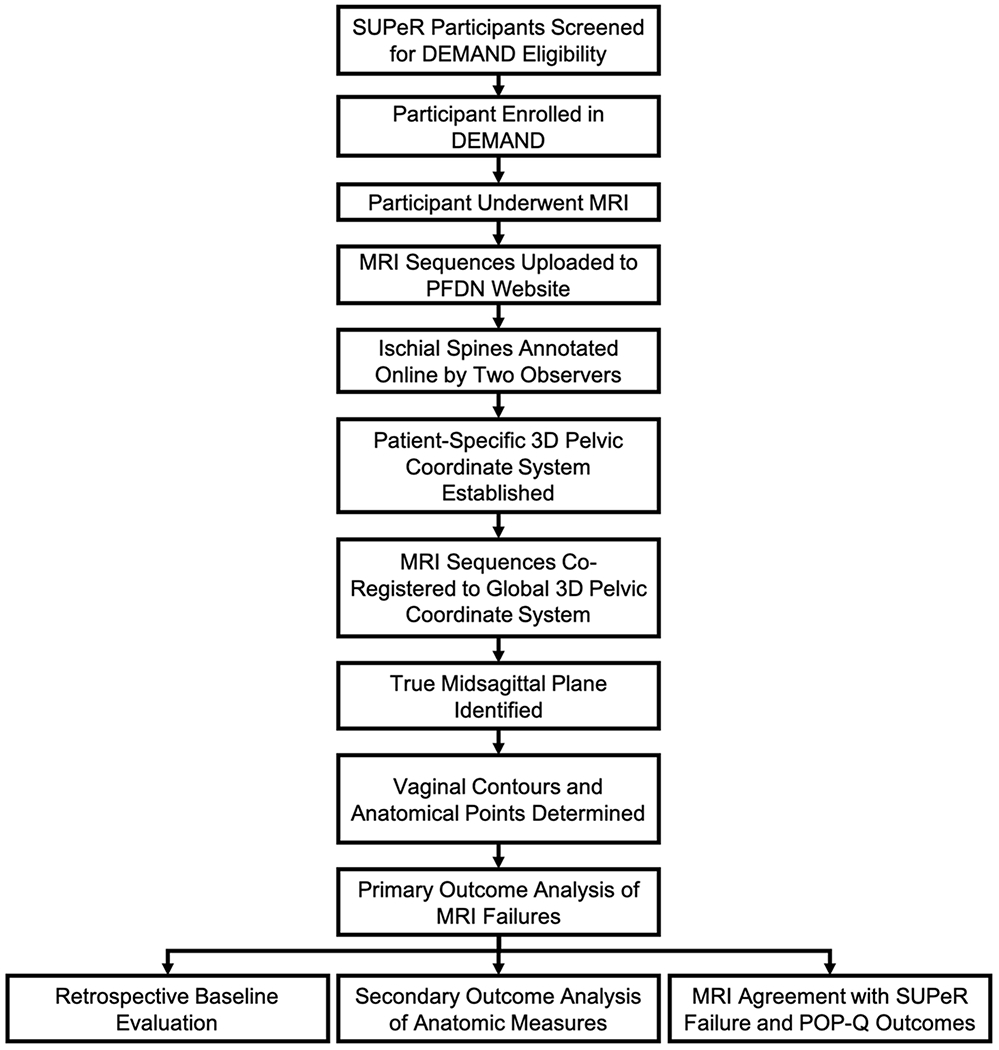
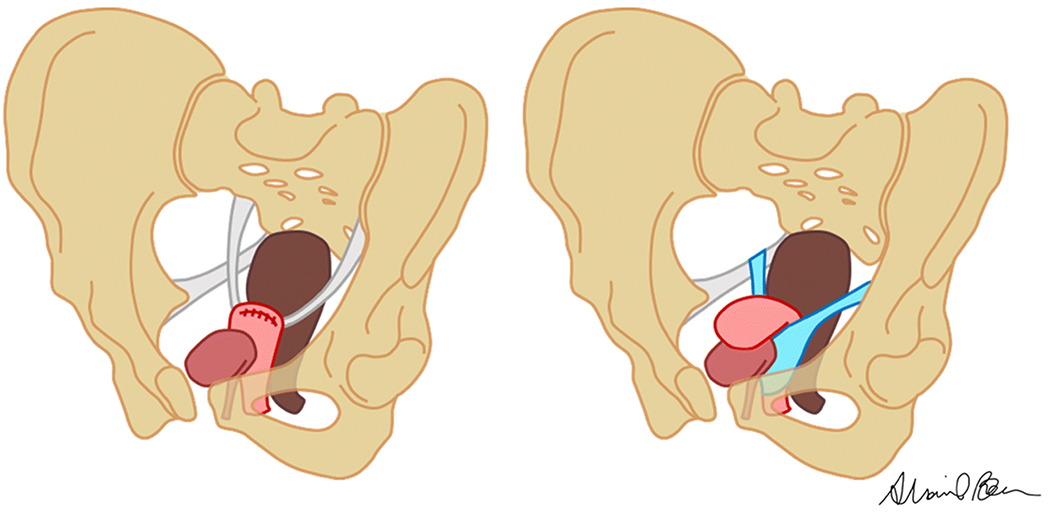
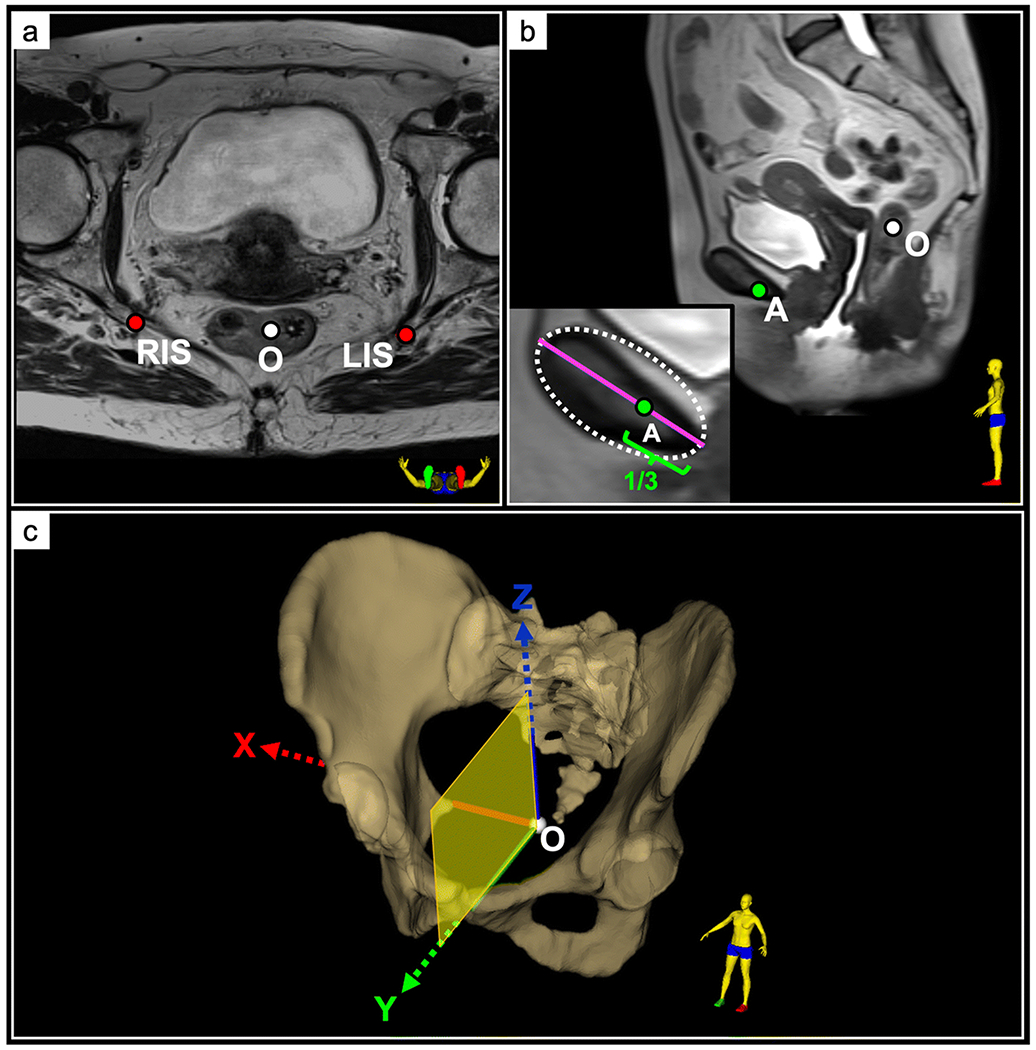
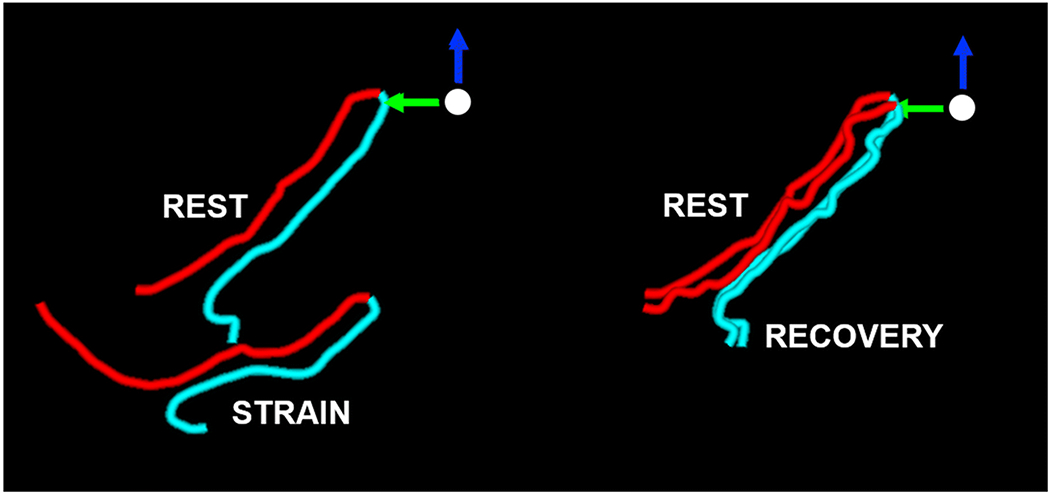
Methods: DEMAND is a supplementary cohort study of a clinical trial in which women with uterovaginal prolapse randomized to (1) vaginal hysterectomy with uterosacral ligament suspension or (2) vaginal mesh hysteropexy underwent pelvic magnetic resonance imaging (MRI) at 30-42 months post-surgery. Standardized protocols have been developed to systematize MRI examinations across multiple sites and to improve reliability of MRI measurements. Anatomical failure, based on MRI, is defined as prolapse beyond the hymen. Anatomic measures from co-registered rest, maximal strain, and post-strain rest (recovery) sequences are obtained from the "true mid-sagittal" plane defined by a 3D pelvic coordinate system. The primary outcome is the mechanism of failure (apical descent versus anterior vaginal wall elongation). Secondary outcomes include displacement of the vaginal apex and perineal body and elongation of the anterior wall, posterior wall, perimeter, and introitus of the vagina between (1) rest and strain and (2) rest and recovery.
Results: Recruitment and MRI trials of 94 participants were completed by May 2018.
Conclusions: Methods papers which detail studies designed to evaluate anatomic outcomes of prolapse surgeries are few. We describe a systematic, standardized approach to define and quantitatively assess mechanisms of anatomic failure following prolapse repair. This study will provide a better understanding of how apical prolapse repairs fail anatomically.
Keywords: Hysteropexy; MRI; Pelvic organ prolapse; Prolapse surgery; Transvaginal mesh; Vaginal hysterectomy.
Conflict of interest statement
DISCLOSURES:
Pamela A. Moalli: Amphora Medical Inc, consulting; NICHD, research support;
Shaniel T. Bowen: None
Steven D. Abramowitch: NICHD: research support;
Mark E. Lockhart: JUM, deputy editor, salary and editorial work; Elsevier, book royalties; Oxford Publishers, book royalties;
Michael Ham: None
Michael E. Hahn: General Electric, research grant; HealthLytix, consultant;
Alison C. Weidner: OBGYN Survey, assistant editor, salary and editorial work; NICHD, research support; Urocure, consultant.
Holly E. Richter: IUJ, OG, editorial work and travel reimbursement; Worldwide Fistula Fund, board membership and travel reimbursement; American Urogynecologic Society, Board of Directors, travel reimbursement; Bluewind, DSMB; Renovia, Allergan, NICHD, NIA, research support; UpToDate, licensor and royalties;
Charles R. Rardin: FPMRS, editorial board membership; Solace Therapeutics, Pelvalon, Foundation for Female Health Awareness, NICHD, research support;
Yuko M. Komesu: Cook-Myosite®, funding; NICHD, funding
Heidi S. Harvie: None
Beri M. Ridgeway: Coloplast Corp, consulting, education, and travel & lodging;
Donna Mazloomdoost: Boston Scientific, research grant
Amanda Shaffer: None
Marie G. Gantz: Boston Scientific, research grant
Figures
References
Publication types
MeSH terms
Grants and funding
- U10 HD041261/HD/NICHD NIH HHS/United States
- UG1 HD069013/HD/NICHD NIH HHS/United States
- U10 HD054215/HD/NICHD NIH HHS/United States
- U10 HD054214/HD/NICHD NIH HHS/United States
- UG1 HD069006/HD/NICHD NIH HHS/United States
- UG1 HD069025/HD/NICHD NIH HHS/United States
- U01 HD069031/HD/NICHD NIH HHS/United States
- U10 HD041267/HD/NICHD NIH HHS/United States
- UG1 HD041267/HD/NICHD NIH HHS/United States
- UG1 HD054215/HD/NICHD NIH HHS/United States
- 5T32EB003392-13/EB/NIBIB NIH HHS/United States
- U10 HD069025/HD/NICHD NIH HHS/United States
- T32 EB003392/EB/NIBIB NIH HHS/United States
- UG1 HD069010/HD/NICHD NIH HHS/United States
- U10 HD069013/HD/NICHD NIH HHS/United States
- UG1 HD054214/HD/NICHD NIH HHS/United States
- U10 HD069006/HD/NICHD NIH HHS/United States
- U10 HD069010/HD/NICHD NIH HHS/United States
- UG1 HD041261/HD/NICHD NIH HHS/United States
- U24 HD069031/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
