

Readmissions Reduction Program: Mortality and Readmissions for Chronic Obstructive Pulmonary Disease
- PMID: 32871097
- PMCID: PMC7885833
- DOI: 10.1164/rccm.202002-0310OC
Readmissions Reduction Program: Mortality and Readmissions for Chronic Obstructive Pulmonary Disease
Abstract
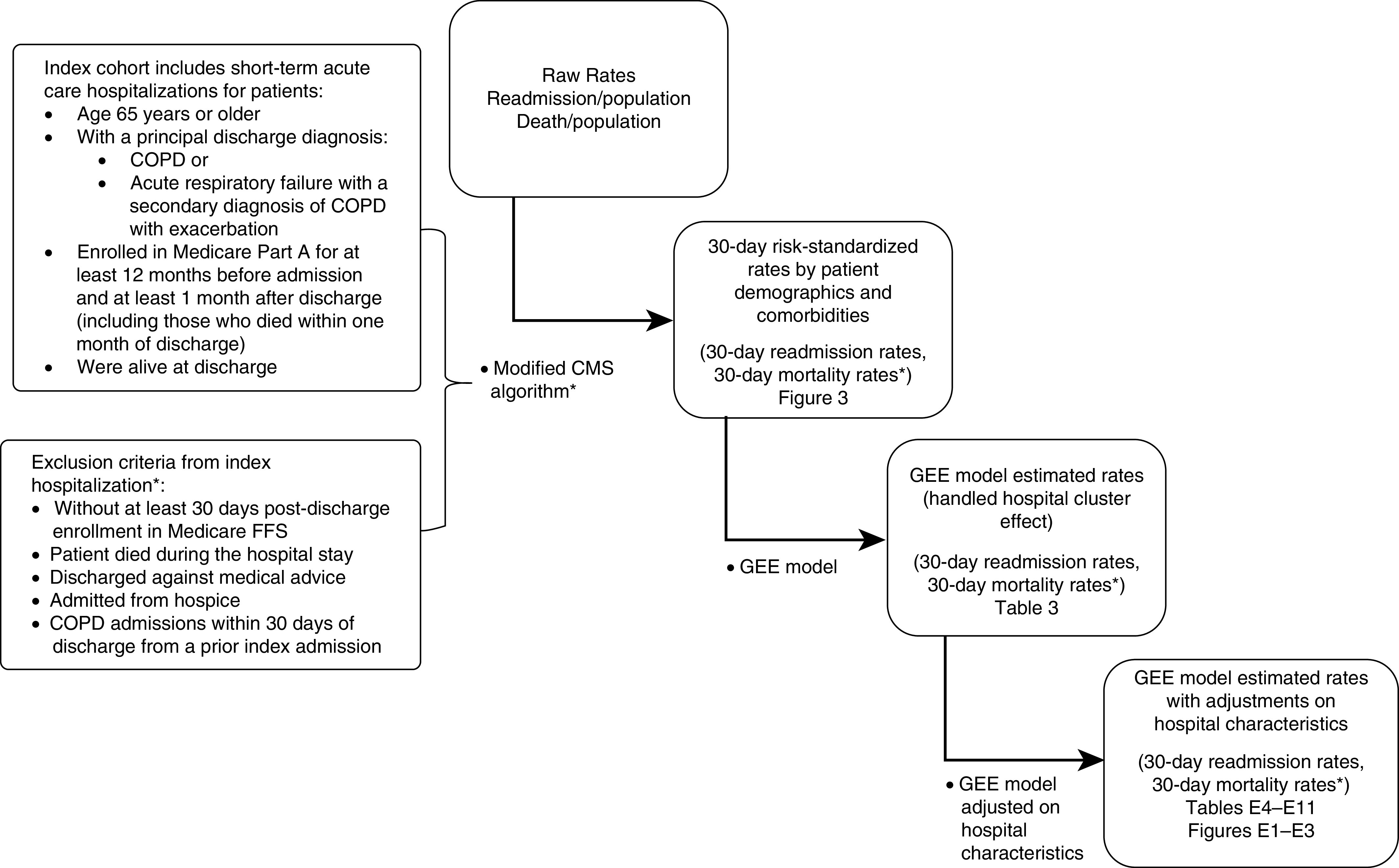
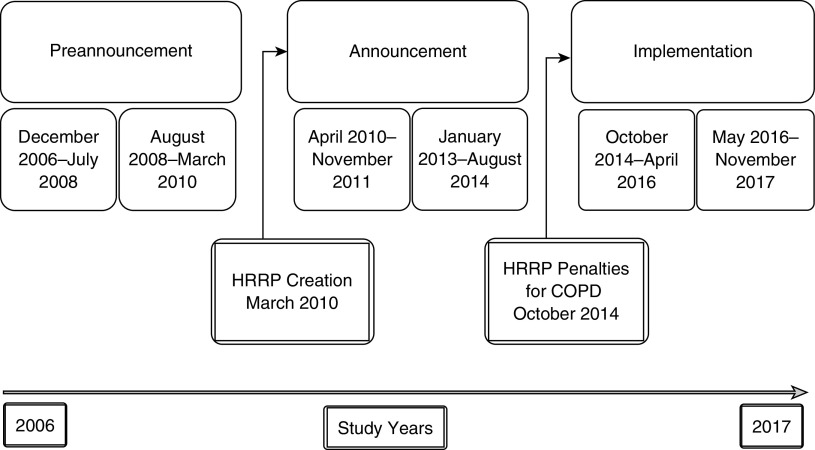
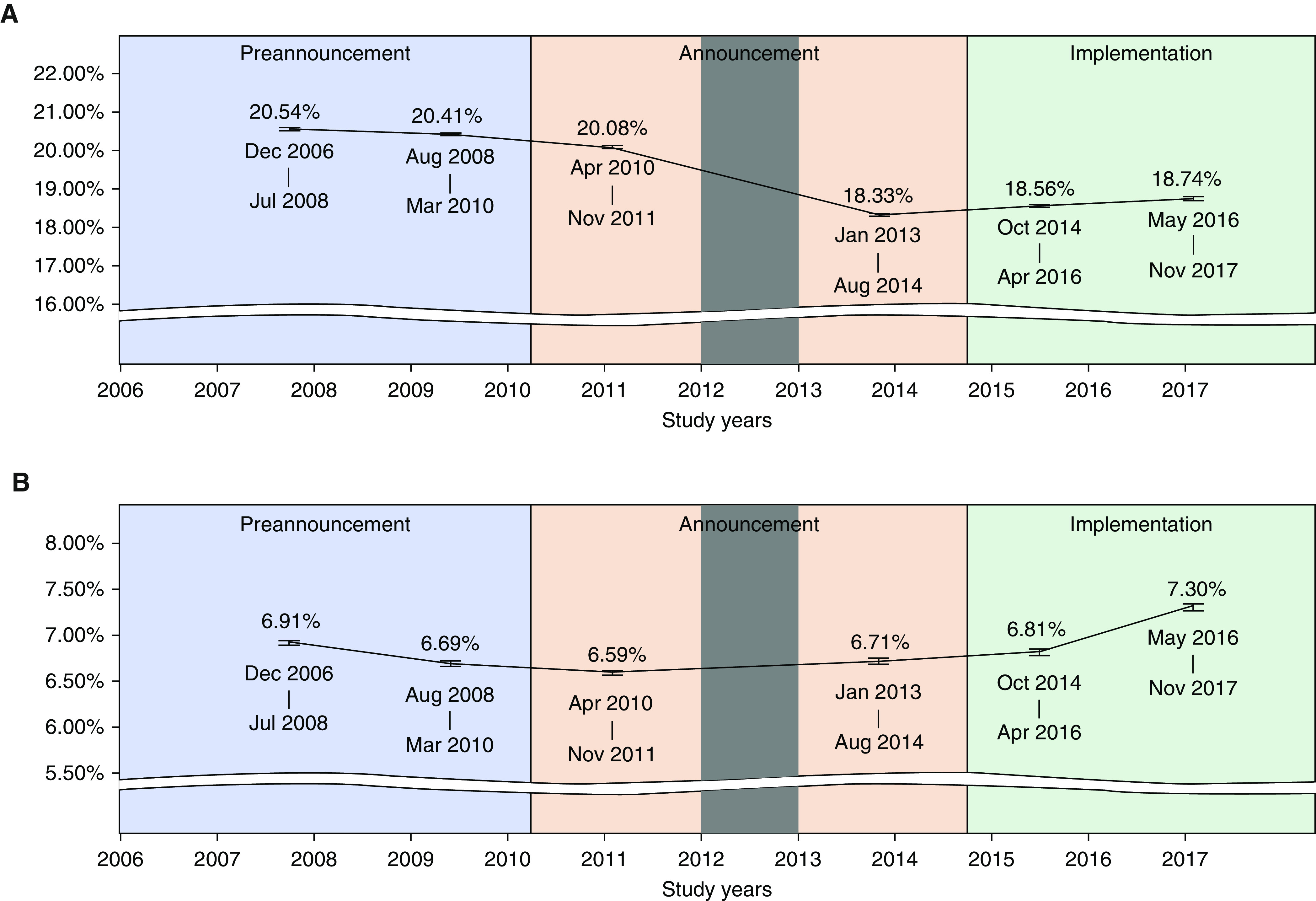
Rationale: Implementation of the Hospital Readmissions Reduction Program (HRRP) following discharge of patients with chronic obstructive pulmonary disease (COPD) has led to a reduction in 30-day readmissions with unknown effects on postdischarge mortality.Objectives: To examine the association of HRRP with 30-day hospital readmission and 30-day postdischarge mortality rate in patients after discharge from COPD hospitalization.Methods: Retrospective cohort study of readmission and mortality rates in a national cohort (N = 4,587,542) of admissions of Medicare fee-for-service beneficiaries 65 years or older with COPD from 2006 to 2017.Measurements and Main Results: Data were analyzed for three nonoverlapping periods based on implementation of the HRRP specific to COPD: 1) preannouncement (December 2006 to March 2010), 2) announcement (April 2010 to August 2014), and 3) implementation (October 2014 to November 2017). The 30-day readmission rate decreased from 20.54% in the preannouncement period (December 2006 to July 2008) to 18.74% in the implementation period (May 2016 to November 2017). The 30-day risk-standardized postdischarge mortality rates were 6.91%, 6.59%, and 7.30% for the preannouncement, announcement, and implementation periods, respectively. Generalized estimating equations analyses estimated an additional 1,196 deaths (October 2014 to April 2016) and 3,858 deaths (May 2016 to November 2017) during the HRRP implementation period.Conclusions: We found a reduction in 30-day all-cause readmission rate during the implementation period compared with the preannouncement phase. HRRP implementation was also associated with a significant increase in 30-day mortality after discharge from COPD hospitalization. Additional research is necessary to confirm our findings and understand the factors contributing to increased mortality in patients with COPD in the HRRP implementation period.
Keywords: Medicare; hospital readmissions; hospitalization; mortality; obstructive lung diseases.
Figures
Comment in
-
Time to Revisit the Hospital Readmissions Reduction Program for Patients Hospitalized for Chronic Obstructive Pulmonary Disease Exacerbations.Am J Respir Crit Care Med. 2021 Feb 15;203(4):403-404. doi: 10.1164/rccm.202009-3392ED. Am J Respir Crit Care Med. 2021. PMID: 32946283 Free PMC article. No abstract available.
-
Apparent Increase in Chronic Obstructive Pulmonary Disease Mortality Is Likely an Artifact of Changes in Documentation and Coding.Am J Respir Crit Care Med. 2021 Mar 1;203(5):647-649. doi: 10.1164/rccm.202009-3697LE. Am J Respir Crit Care Med. 2021. PMID: 33166177 Free PMC article. No abstract available.
-
Reply to Lindenauer et al.: Apparent Increase in Chronic Obstructive Pulmonary Disease Mortality Is Likely an Artifact of Changes in Documentation and Coding.Am J Respir Crit Care Med. 2021 Mar 1;203(5):649-651. doi: 10.1164/rccm.202010-3855LE. Am J Respir Crit Care Med. 2021. PMID: 33166199 Free PMC article. No abstract available.
References
-
- Murphy SL, Xu J, Kochanek KD, Arias E. Mortality in the United States, 2017. NCHS Data Brief. 2018;328:1–8. - PubMed
-
- Wier LM, Elixhauser A, Pfuntner A, Au DH. Rockville, MD: Agency for Health Care Policy and Research; 2006. Overview of hospitalizations among patients with COPD, 2008: statistical brief# 106. In: Healthcare cost and Utilization Project (HCUP) statistical briefs. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
