

The efficacy and safety of the infiltration of the interspace between the popliteal artery and the capsule of the knee block in total knee arthroplasty: A prospective randomized trial protocol
- PMID: 32872033
- PMCID: PMC7437726
- DOI: 10.1097/MD.0000000000021670
The efficacy and safety of the infiltration of the interspace between the popliteal artery and the capsule of the knee block in total knee arthroplasty: A prospective randomized trial protocol
Expression of concern in
-
Expression of Concern: Study Protocols.Medicine (Baltimore). 2025 Nov 7;104(45):e46330. doi: 10.1097/MD.0000000000046330. Medicine (Baltimore). 2025. PMID: 41204616 Free PMC article. No abstract available.
Abstract
Background: Total knee arthroplasty (TKA) is an established and successful surgical procedure which is the major treatment for degenerative knee joint diseases. A novel technique to address posterior knee joint pain is the infiltration of local anesthetic between the interspace between the popliteal artery and capsule of the knee (IPACK). The goal of this randomized clinical trial was to assess the efficacy and safety of adding IPACK to adductor canal block (ACB) after TKA.
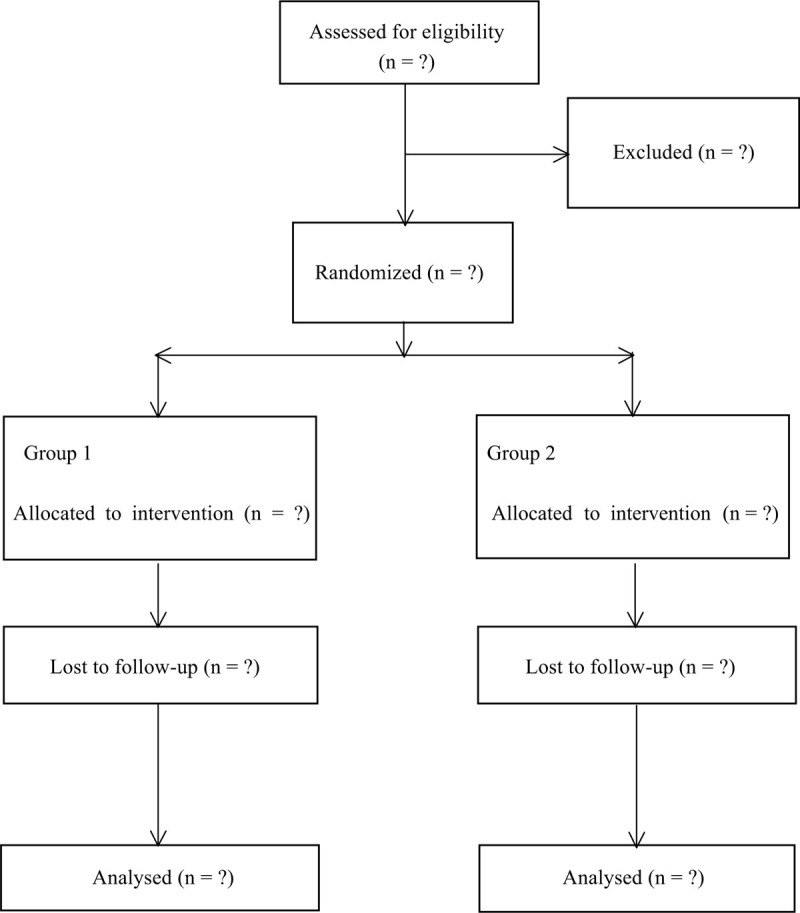
Methods: This was a prospectively randomized trial that investigated the effectiveness and safety of the IPACK after TKA. Approval from Clinical Studies Ethical Committee in Qilu Hospital of Shandong University was obtained. The inclusion criteria were adult patients undergoing primary unilateral TKA and American Society of Anesthesiologists grade 1 or 2 with normal cognitive function. The patients were randomized to 1 of 2 treatment options: ACB-alone group and ACB + IPACK group. The primary outcome was the total morphine consumption during postoperative 24 hours. Secondary outcomes included postoperative pain score, time to first and total dosage of rescue morphine in postoperative 48 hours, early and late postoperative period (from postoperative day 0-3 months follow-up) performance-based test (Timed-Up and Go test, and quadriceps strength). Postoperative nausea and vomiting, length of hospital stay, patient satisfaction, and other adverse events were also evaluated.
Results: It was hypothesized that when combined with a control group, the IPACK block would result in a lower morphine consumption and pain score after TKA.
Trial registration: This study protocol was registered in Research Registry (researchregistry5765).
Conflict of interest statement
The authors have no conflicts of interest to disclose.
References
-
- Li S, Luo X, Wang P, et al. Clinical outcomes of gap balancing vs measured resection in total knee arthroplasty: a systematic review and meta-analysis involving 2259 subjects. J Arthroplasty 2018;33:2684–93. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
