Prevalence of tumor BRCA1 and BRCA2 dysfunction in unselected patients with ovarian cancer
- PMID: 32872764
- PMCID: PMC7494761
- DOI: 10.5468/ogs.20033
Prevalence of tumor BRCA1 and BRCA2 dysfunction in unselected patients with ovarian cancer
Abstract
Objective: The therapeutic benefits of poly(ADP-ribose) polymerase inhibitors highlight the need to evaluate BRCA1/2 defects in tubal/ovarian cancer (OC). We sought to determine the pattern and disease characteristics associated with tumor BRCA1/2 mutations and BRCA1 methylation in women with OC.
Methods: We obtained 111 OC specimens from 2 university hospitals and assessed BRCA1/2 mutations and BRCA1 methylation in tumor DNA. The frequency and pattern of BRCA1/2 defects were examined. Associations between patient/disease characteristics and BRCA1/2 defects were ascertained (Fisher's exact test). Platinum-free interval (PFI), progression-free survival (PFS), and overall survival (OS) based on the underlying BRCA1/2 defect were determined (Kaplan-Meier analysis [log-rank test]).
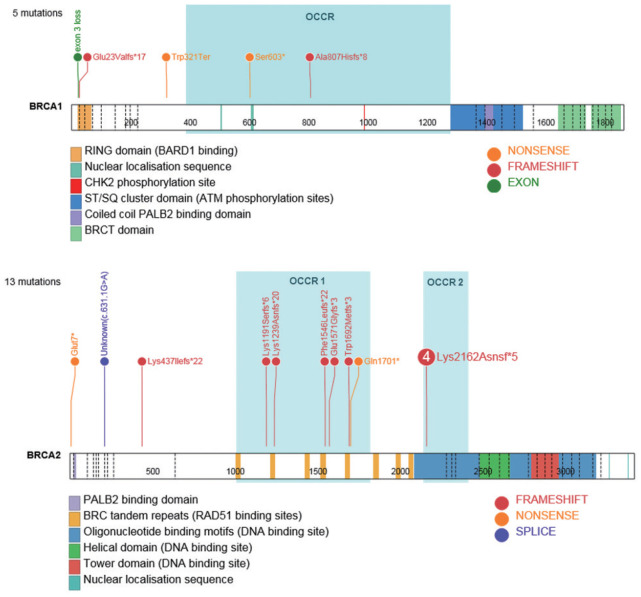
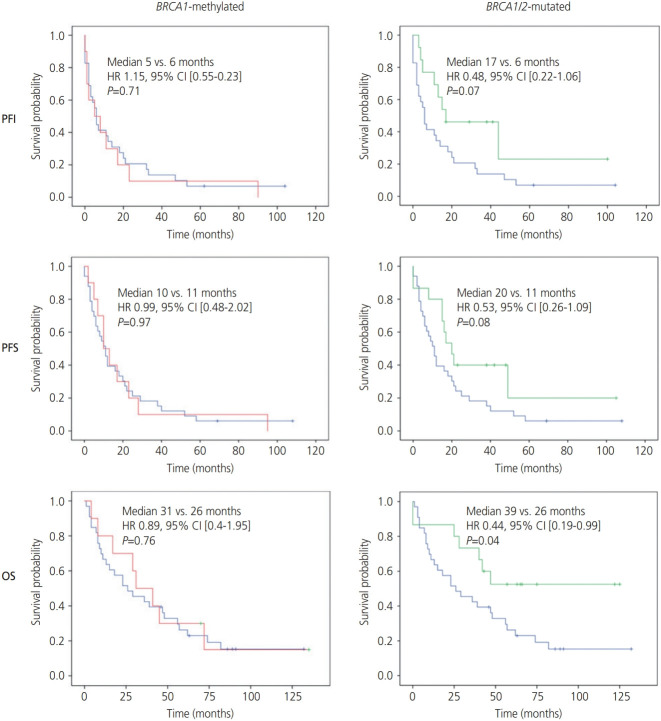
Results: We observed a BRCA1/2 dysfunction rate of 40% (28/70) in high-grade serous tubal/ovarian cancer (HGSC), including 14.3% BRCA1 methylation (n=10), 7.1% BRCA1 mutation (n=5), and 18.6% BRCA2 mutation (n=13). Defects in BRCA1/2 genes were associated with stage III/IV HGSC (BRCA1 methylation: P=0.005 [stage III/IV] and P=0.004 [HGSC]; BRCA1/2 mutation: P=0.03 [stage III/IV] and P<0.001 [HGSC]). Patients with BRCA1/2-mutated cancers showed improved OS (hazard ratio [HR], 0.65; 95% confidence interval [CI], 0.43-0.99; P=0.045) and a trend toward improved PFI (HR, 0.48; 95% CI, 0.22-1.06; P=0.07) and PFS (HR, 0.72; 95% CI, 0.51-1.03; P=0.07). No survival differences were observed between BRCA1-methylated and BRCA1/2 wild-type non-BRCA1-methylated cancers.
Conclusion: We observed a high tumor BRCA1/2 dysfunction rate in HGSC with a unique predominance of BRCA2 over BRCA1 mutations. While BRCA1/2 mutations conferred survival benefits in OC, no such association was observed with BRCA1 methylation.
Keywords: BRCA1 methylation; BRCA1 mutation; BRCA2 mutation; Ovarian cancer.
Conflict of interest statement
Roshni D. Kalachand has received conference travel fees from Astra Zeneca. Kirsten M. Timms is an employee of and may hold shares in Myriad Genetics Inc. The other authors have no conflicts of interest to declare.
Figures
References
-
- Mirza MR, Monk BJ, Herrstedt J, Oza AM, Mahner S, Redondo A, et al. Niraparib maintenance therapy in platinum-sensitive, recurrent ovarian cancer. N Engl J Med. 2016;375:2154–64. - PubMed
-
- Swisher EM, Lin KK, Oza AM, Scott CL, Giordano H, Sun J, et al. Rucaparib in relapsed, platinum-sensitive high-grade ovarian carcinoma (ARIEL2 Part 1): an international, multicentre, open-label, phase 2 trial. Lancet Oncol. 2017;18:75–87. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous