

Ketamine to treat super-refractory status epilepticus
- PMID: 32873691
- PMCID: PMC7713785
- DOI: 10.1212/WNL.0000000000010611
Ketamine to treat super-refractory status epilepticus
Abstract
Objective: To test ketamine infusion efficacy in the treatment of super-refractory status epilepticus (SRSE), we studied patients with SRSE who were treated with ketamine retrospectively. We also studied the effect of high doses of ketamine on brain physiology as reflected by invasive multimodality monitoring (MMM).
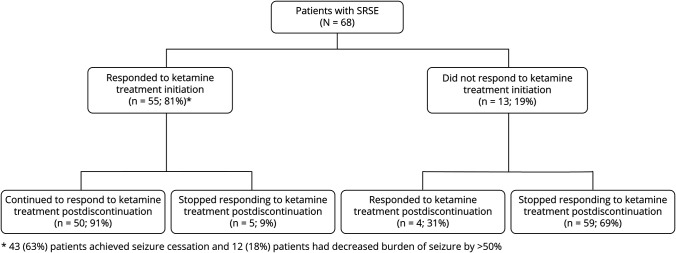
Methods: We studied a consecutive series of 68 patients with SRSE who were admitted between 2009 and 2018, treated with ketamine, and monitored with scalp EEG. Eleven of these patients underwent MMM at the time of ketamine administration. We compared patients who had seizure cessation after ketamine initiation to those who did not.
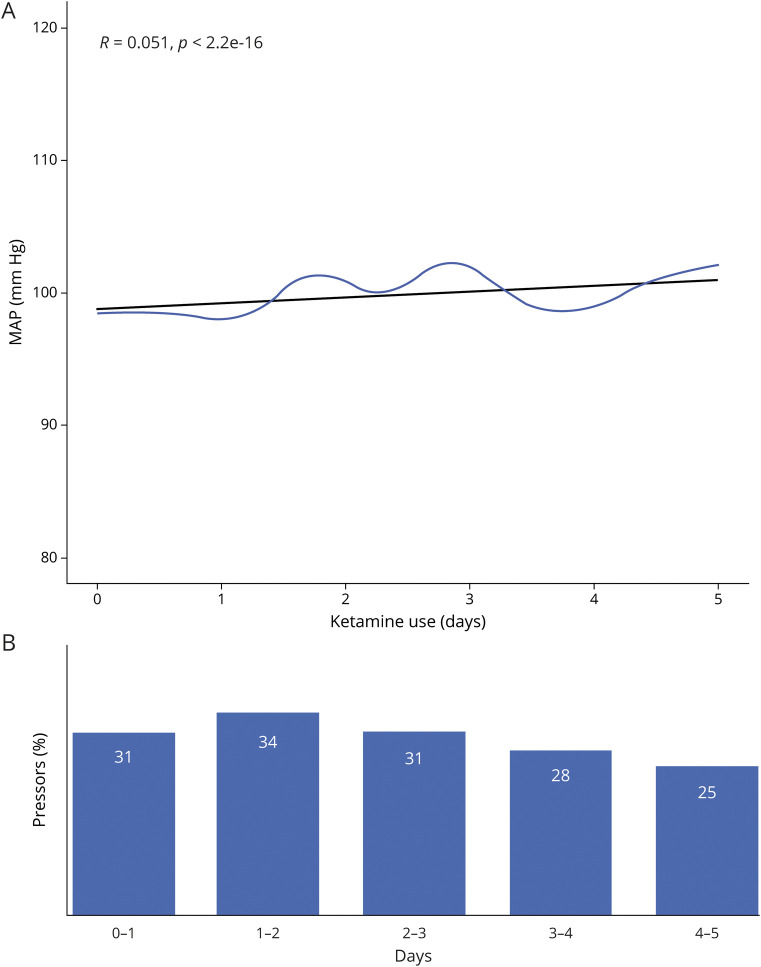
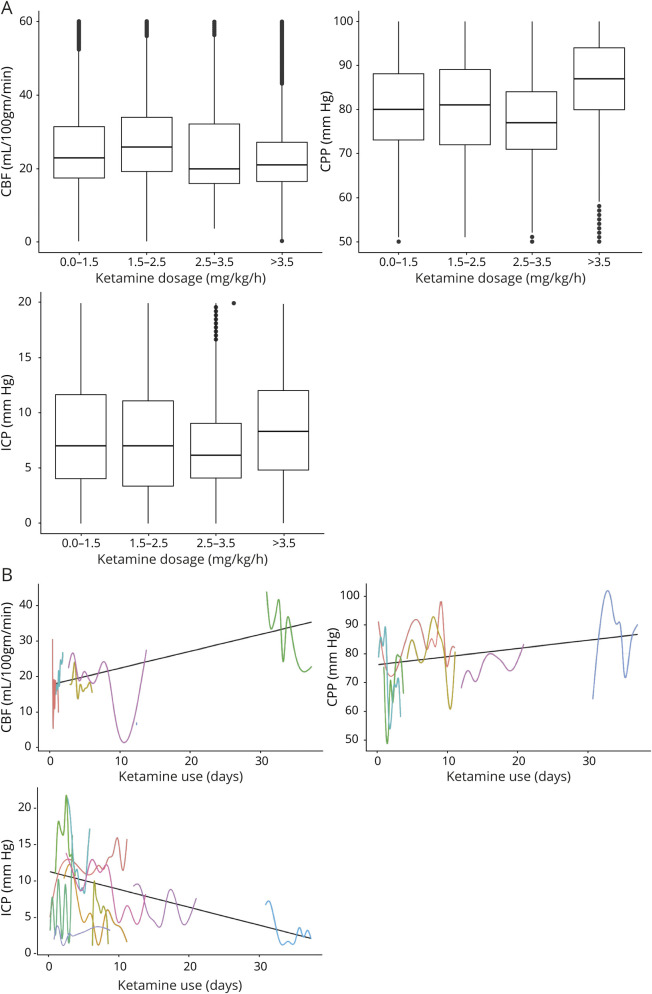
Results: Mean age was 53 ± 18 years and 46% of patients were female. Seizure burden decreased by at least 50% within 24 hours of starting ketamine in 55 (81%) patients, with complete cessation in 43 (63%). Average dose of ketamine infusion was 2.2 ± 1.8 mg/kg/h, with median duration of 2 (1-4) days. Average dose of midazolam was 1.0 ± 0.8 mg/kg/h at the time of ketamine initiation and was started at a median of 0.4 (0.1-1.0) days before ketamine. Using a generalized linear mixed effect model, ketamine was associated with stable mean arterial pressure (odds ratio 1.39, 95% confidence interval 1.38-1.40) and with decreased vasopressor requirements over time. We found no effect on intracranial pressure, cerebral blood flow, or cerebral perfusion pressure.
Conclusion: Ketamine treatment was associated with a decrease in seizure burden in patients with SRSE. Our data support the notion that high-dose ketamine infusions are associated with decreased vasopressor requirements without increased intracranial pressure.
Classification of evidence: This study provides Class IV evidence that ketamine decreases seizures in patients with SRSE.
© 2020 American Academy of Neurology.
Figures
Comment in
-
Super K for Super-R(efractory) Status Epilepticus: Bringing Down Seizures While Keeping Up Blood Pressure With Ketamine.Epilepsy Curr. 2020 Dec 17;21(1):36-39. doi: 10.1177/1535759720975740. eCollection 2021 Jan-Feb. Epilepsy Curr. 2020. PMID: 34025272 Free PMC article. No abstract available.
References
-
- Brophy GM, Bell R, Claassen J, et al. . Guidelines for the evaluation and management of status epilepticus. Neurocrit Care 2012;17:3–23. - PubMed
-
- Chen JW, Wasterlain CG. Status epilepticus: pathophysiology and management in adults. Lancet Neurol 2006;5:246–256. - PubMed
-
- Prüss H, Holtkamp M. Ketamine successfully terminates malignant status epilepticus. Epilepsy Res 2008;82:219–222. - PubMed
-
- Sheth RD, Gidal BE. Refractory status epilepticus: response to ketamine. Neurology 1998;51:1765–1766. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials