

Preserved Ratio Impaired Spirometry in a Spirometry Database
- PMID: 32873751
- PMCID: PMC7856524
- DOI: 10.4187/respcare.07712
Preserved Ratio Impaired Spirometry in a Spirometry Database
Abstract
Background: Spirometry results can yield a diagnosis of normal air flow, air flow obstruction, or preserved ratio impaired spirometry (PRISm), defined as a reduced FEV1 or FVC in the setting of preserved FEV1/FVC. Previous studies have estimated the prevalence of PRISm to be 7-12%. Our objective was to examine the prevalence of PRISm in a spirometry database and to identify factors associated with PRISm.
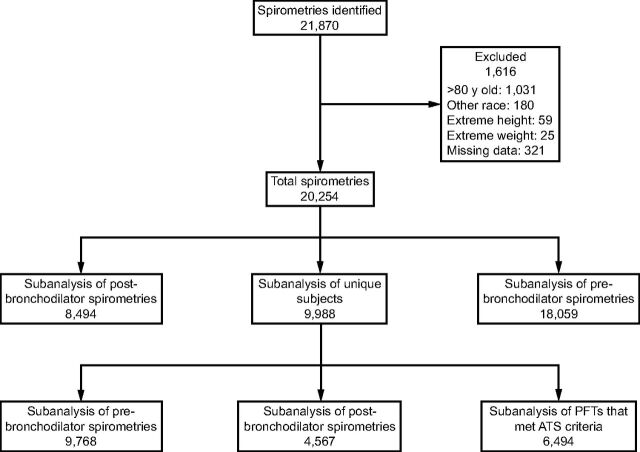
Methods: We performed a retrospective analysis of 21,870 spirometries; 1,616 were excluded because of missing data or extremes of age, height, or weight. We calculated the prevalence of PRISm in prebronchodilator and postbronchodilator pulmonary function tests. Subsequently, we calculated the prevalence of PRISm by various age, race, body mass index, and diagnosis categories, as well as by gender and smokers versus nonsmokers. Finally, in the subset of the cohort with FEV1 < lower limit of normal, we performed a multivariable logistic regression analysis to identify factors associated with PRISm.
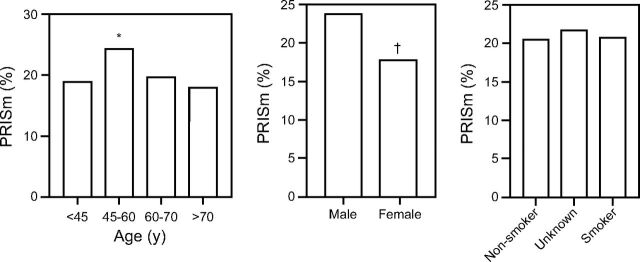
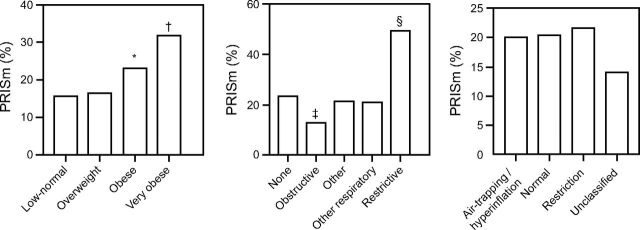
Results: We identified 18,059 prebronchodilator spirometries, and 22.3% of these yielded a PRISm diagnosis. This prevalence remained stable in postbronchodilator spirometries (17.7%), after excluding earlier pulmonary function tests for subjects with multiple pulmonary function tests (20.7% in prebronchodilator and 24.3% in postbronchodilator), and when we limited the analysis to prebronchodilator spirometries that met American Thoracic Society criteria (20.6%). The PRISm prevalence was higher in subjects 45-60 y old (24.4%) and in males (23.7%) versus females (17.9%). The prevalence rose with body mass index and was higher for those with a referral diagnosis of restrictive lung disease (50%). PRISm prevalence was similar between races and smokers versus nonsmokers. In a multivariable analysis, higher % of predicted FEV1 (odds ratio 1.51, 95% CI 1.42-1.60), body mass index (odds ratio 1.52, 95% CI 1.39-1.68), and restrictive lung disease (odds ratio 4.32, 95% CI 2.54-7.57) were associated with a diagnosis of PRISm. Smoking was inversely associated (odds ratio 0.55, 95% CI 0.46-0.65) with PRISm.
Conclusions: In a spirometry database at an academic medical center, the PRISm prevalence was 17-24%, which is higher than previously reported.
Keywords: chronic obstructive pulmonary disease; lung volume measurements; plethysmography; preserved ratio impaired spirometry (PRISm); respiratory function tests; spirometry.
Copyright © 2021 by Daedalus Enterprises.
Figures
References
-
- Mannino DM, Doherty DE, Buist AS. Global Initiative on Obstructive Lung Disease (GOLD) classification of lung disease and mortality: findings from the Atherosclerosis Risk in Communities (ARIC) study. Respir Med 2006;100(1):115–122. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
