

Laser interstitial thermal therapy in neuro-oncology applications
- PMID: 32874734
- PMCID: PMC7451173
- DOI: 10.25259/SNI_496_2019
Laser interstitial thermal therapy in neuro-oncology applications
Abstract
Background: Laser interstitial thermal therapy (LITT) is a minimally invasive surgical treatment for multiple intracranial pathologies that are of growing interest to neurosurgeons and their patients and is emerging as an effective alternative to standard of care open surgery in the neurosurgical armamentarium. This option was initially considered for those patients with medical comorbidities and lesion-specific characteristics that confer excessively high risk for resection through a standard craniotomy approach but indications are changing.
Methods: The PubMed database was searched for studies in the English literature on LITT for the treatment of primary and metastatic brain tumors, meningiomas, as well as for radiation necrosis (RN) in previously irradiated brain tumors.
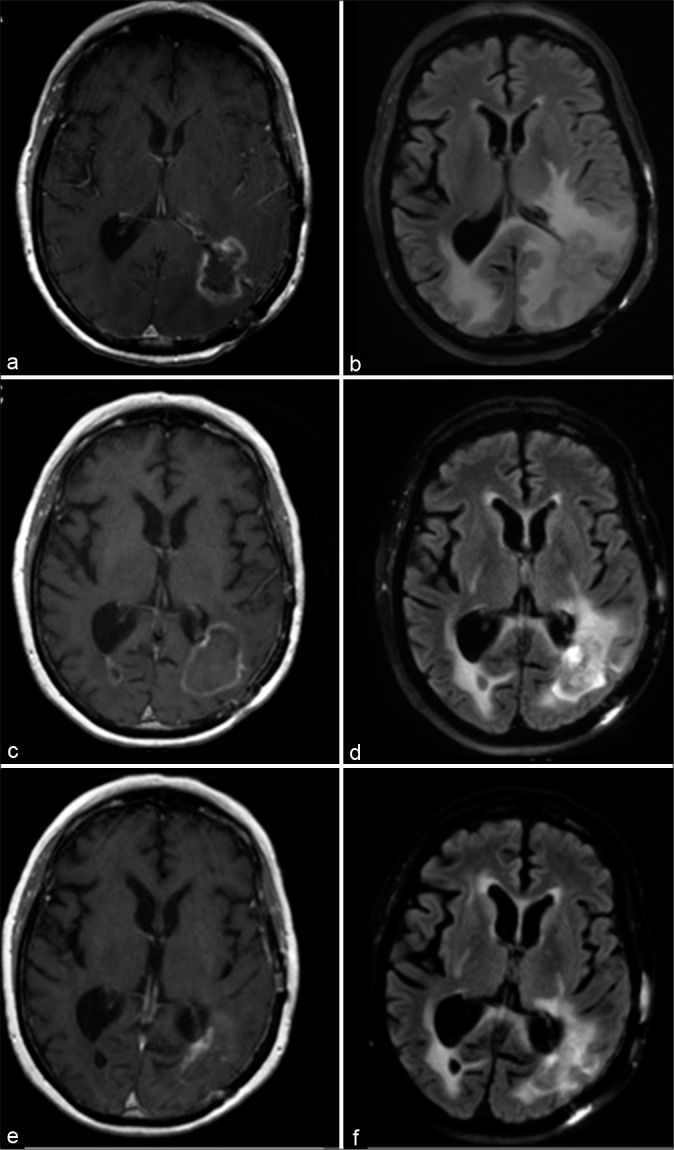
Results: This review provides an update of the relevant literature regarding application of LITT in neurosurgical oncology for the treatment of de novo and recurrent primary gliomas and brain metastases radiographically regrowing after previous irradiation as recurrent tumor or RN. In addition, this review details the limited experience of LITT with meningiomas and symptomatic peritumoral edema after radiosurgery. The advantages and disadvantages, indications, and comparisons to standard of care treatments such as craniotomy for open surgical resection are discussed for each pathology. Finally, the literature on cost-benefit analyses for LITT are reviewed.
Conclusion: The studies discussed in this review have helped define the role of LITT in neurosurgical oncology and delineate optimal patient selection and tumor characteristics most suitable to this intervention.
Keywords: Brain metastasis; Craniotomy; Glioma; Laser interstitial thermal therapy; Meningioma; Radiation necrosis.
Copyright: © 2020 Surgical Neurology International.
Conflict of interest statement
Dr. Chiang is a consultant for Monteris Medical Inc. (Minnesota, USA) and speaker for BrainLab, Inc. (Munich, Germany).
Figures


References
-
- Ahluwalia M, Barnett GH, Deng D, Tatter SB, Laxton AW, Mohammadi AM, et al. Laser ablation after stereotactic radiosurgery: A multicenter prospective study in patients with metastatic brain tumors and radiation necrosis. J Neurosurg. 2018;130:804–11. - PubMed
-
- Ali MA, Carroll KT, Rennert RC, Hamelin T, Chang L, Lemkuil BP, et al. Stereotactic laser ablation as treatment for brain metastases that recur after stereotactic radiosurgery: A multiinstitutional experience. Neurosurg Focus. 2016;41:E11. - PubMed
-
- Barker FG, 2nd, Chang SM, Gutin PH, Malec MK, McDermott MW, Prados MD, et al. Survival and functional status after resection of recurrent glioblastoma multiforme. Neurosurgery. 1998;42:709–20. discussion 720-3. - PubMed
-
- Barnett GH, Voigt JD, Alhuwalia MS. A systematic review and meta-analysis of studies examining the use of brain laser interstitial thermal therapy versus craniotomy for the treatment of high-grade tumors in or near areas of eloquence: An examination of the extent of resection and major complication rates associated with each type of surgery. Stereotact Funct Neurosurg. 2016;94:164–73. - PubMed
-
- Bastos DC, Rao G, Oliva IC, Loree JM, Fuentes DT, Stafford RJ, et al. Predictors of local control of brain metastasis treated with laser interstitial thermal therapy. Neurosurgery. 2020;87:112–22. - PubMed
Publication types
LinkOut - more resources
Full Text Sources