

Extra-articular Portion of the Sacroiliac Joint-Between the Sacral and Pelvic Tuberosities: An Anatomical Guide for the S2-Alar-Iliac Screw Trajectory
- PMID: 32875863
- PMCID: PMC8013944
- DOI: 10.1177/2192568220903033
Extra-articular Portion of the Sacroiliac Joint-Between the Sacral and Pelvic Tuberosities: An Anatomical Guide for the S2-Alar-Iliac Screw Trajectory
Abstract
Study design: A novel technique for S2-alar-iliac (S2AI) screw placement was analyzed.
Objectives: Accurate confirmation of the S2AI screw trajectory with free-hand techniques is not simple, although some anatomical landmarks have been reported. To overcome the drawback, we aimed to introduce our technique for S2AI screw placement assisted with a guidewire using a new anatomical landmark.
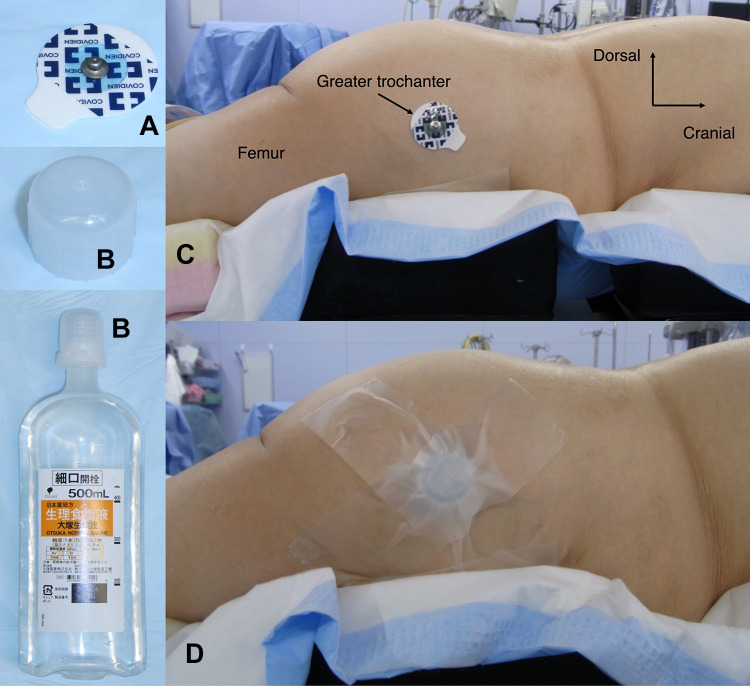
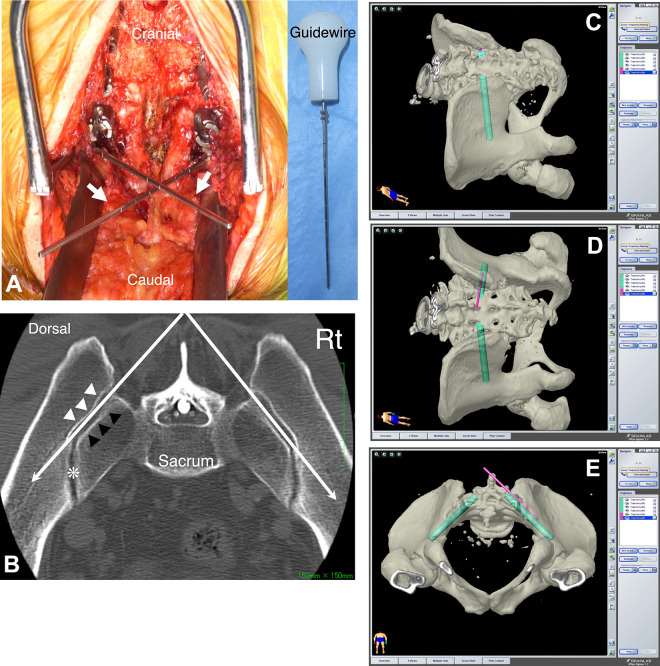
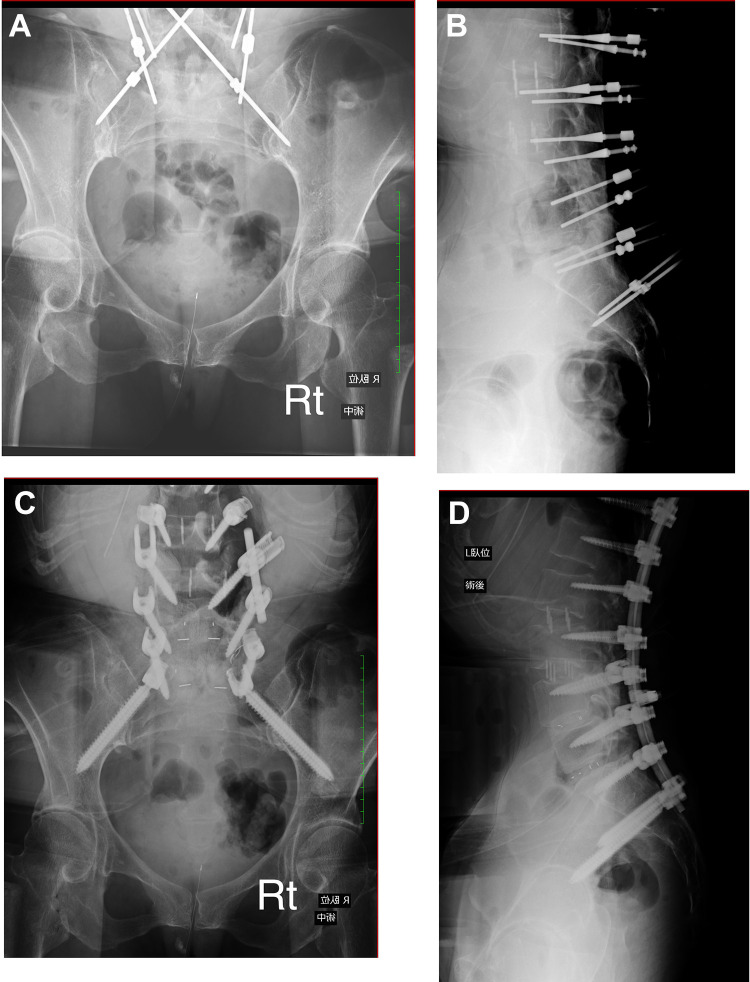
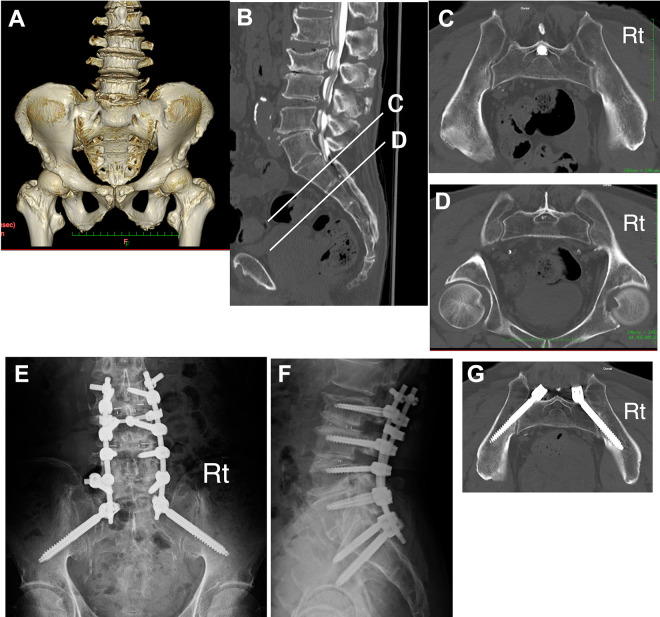
Methods: A total of 104 S2AI screws of 52 patients who underwent S2AI screw placement were investigated. Navigation software was used to simulate S2AI screw placement preoperatively. Screw placement was performed with the nonfluoroscopic free-hand technique. In this technique, a guidewire is inserted into the ilium from the extra-articular portion of the sacroiliac joint just lateral to the ideal screw entry point toward the tip of the greater trochanter and guides the screw trajectory. If the direction of the guidewire is satisfactory, all procedures of screw insertion are performed accordingly. The screw accuracy was assessed with computed tomography.
Results: The modal size of the screw was 9.5 mm × 90 mm. The average horizontal angle was 42.0° (SD = 5.1°) on the right and 40.7° (SD = 4.7°) on the left. Of the 104 screws, 4 screws (3.9%) breached dorsally. No screw-related complication was observed.
Conclusions: Because the guidewire can be inserted at an angle according to the individual morphology of the sacroiliac joint, it will be a reliable guide for the screw trajectory. This technique with a guidewire would help improve the accuracy of S2AI screw placement.
Keywords: S2AI screw; free-hand; lumbosacral transitional vertebra; navigation; spinal deformity; spinopelvic fixation.
Conflict of interest statement
Figures
References
-
- Kebaish KM. Sacropelvic fixation: techniques and complications. Spine (Phila Pa 1976). 2010;35:2245–2251. - PubMed
-
- Sponseller PD, Zimmerman RM, Ko PS, et al. Low profile pelvic fixation with the sacral alar iliac technique in the pediatric population improves results at two-year minimum follow-up. Spine (Phila Pa 1976). 2010;35:1887–1892. - PubMed
-
- Hu X, Lieberman IH. Robotic-guided sacro-pelvic fixation using S2 alar-iliac screws: feasibility and accuracy. Eur Spine J. 2017;26:720–725. - PubMed
-
- O’Brien JR, Yu WD, Bhatnagar R, Sponseller P, Kebaish KM. An anatomic study of the S2 iliac technique for lumbopelvic screw placement. Spine (Phila Pa 1976). 2009;34:E439–E442. - PubMed
LinkOut - more resources
Full Text Sources
