

High Pleural Pressure Prevents Alveolar Overdistension and Hemodynamic Collapse in Acute Respiratory Distress Syndrome with Class III Obesity. A Clinical Trial
- PMID: 32876469
- PMCID: PMC7924574
- DOI: 10.1164/rccm.201909-1687OC
High Pleural Pressure Prevents Alveolar Overdistension and Hemodynamic Collapse in Acute Respiratory Distress Syndrome with Class III Obesity. A Clinical Trial
Abstract
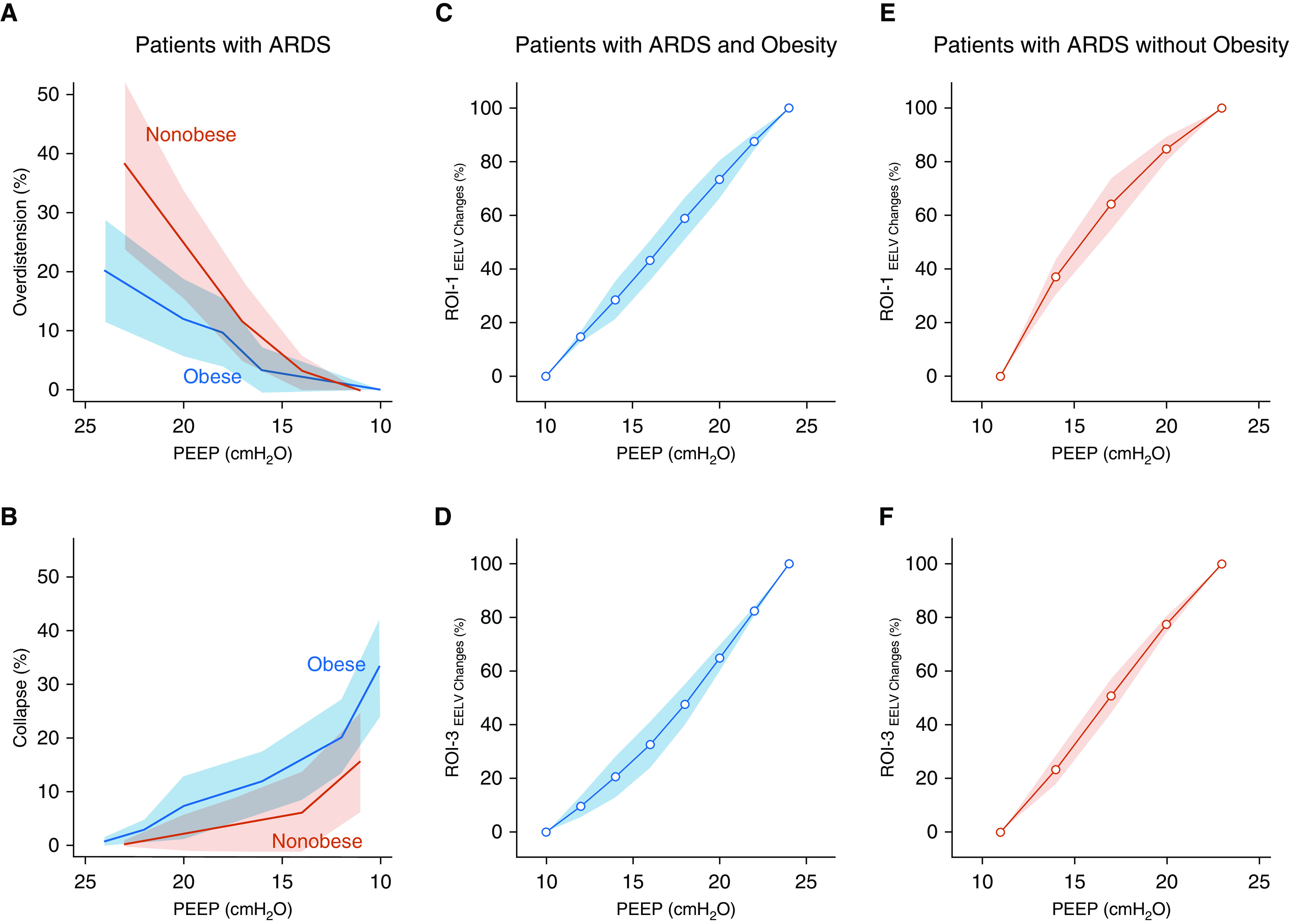
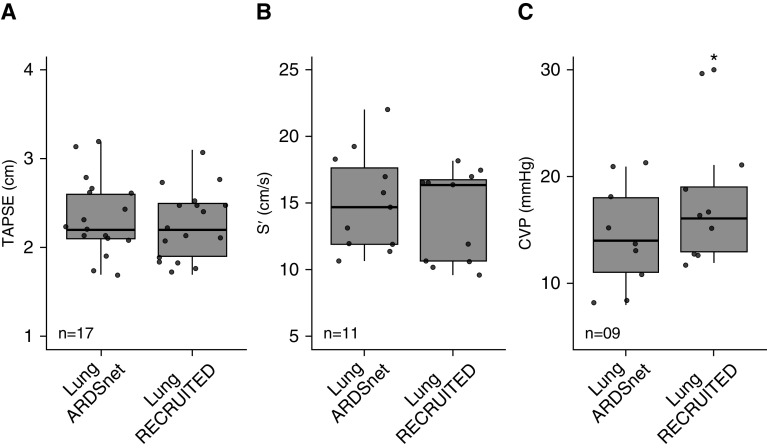
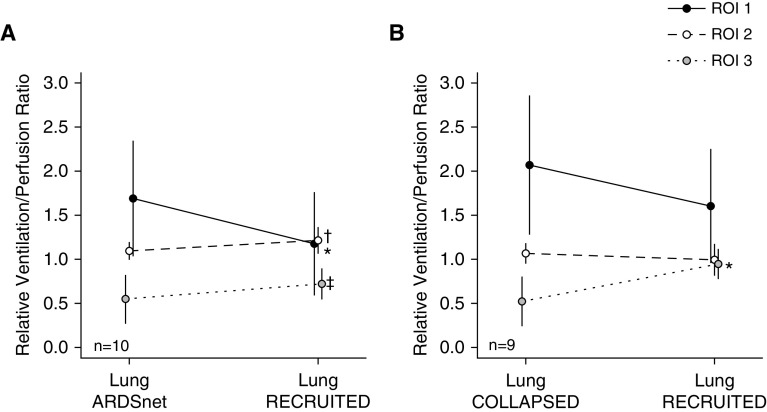
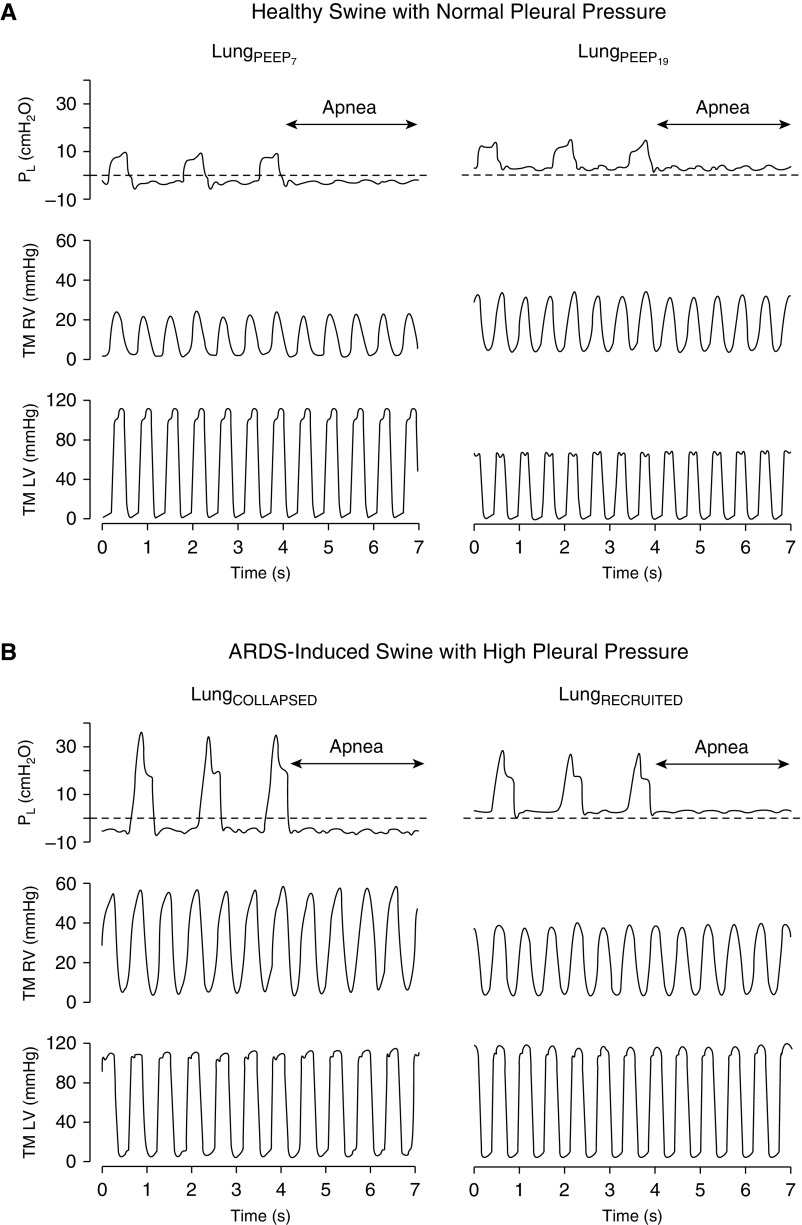
Rationale: Obesity is characterized by elevated pleural pressure (Ppl) and worsening atelectasis during mechanical ventilation in patients with acute respiratory distress syndrome (ARDS).Objectives: To determine the effects of a lung recruitment maneuver (LRM) in the presence of elevated Ppl on hemodynamics, left and right ventricular pressure, and pulmonary vascular resistance. We hypothesized that elevated Ppl protects the cardiovascular system against high airway pressure and prevents lung overdistension.Methods: First, an interventional crossover trial in adult subjects with ARDS and a body mass index ≥ 35 kg/m2 (n = 21) was performed to explore the hemodynamic consequences of the LRM. Second, cardiovascular function was studied during low and high positive end-expiratory pressure (PEEP) in a model of swine with ARDS and high Ppl (n = 9) versus healthy swine with normal Ppl (n = 6).Measurements and Main Results: Subjects with ARDS and obesity (body mass index = 57 ± 12 kg/m2) after LRM required an increase in PEEP of 8 (95% confidence interval [95% CI], 7-10) cm H2O above traditional ARDS Network settings to improve lung function, oxygenation and [Formula: see text]/[Formula: see text] matching, without impairment of hemodynamics or right heart function. ARDS swine with high Ppl demonstrated unchanged transmural left ventricular pressure and systemic blood pressure after the LRM protocol. Pulmonary arterial hypertension decreased (8 [95% CI, 13-4] mm Hg), as did vascular resistance (1.5 [95% CI, 2.2-0.9] Wood units) and transmural right ventricular pressure (10 [95% CI, 15-6] mm Hg) during exhalation. LRM and PEEP decreased pulmonary vascular resistance and normalized the [Formula: see text]/[Formula: see text] ratio.Conclusions: High airway pressure is required to recruit lung atelectasis in patients with ARDS and class III obesity but causes minimal overdistension. In addition, patients with ARDS and class III obesity hemodynamically tolerate LRM with high airway pressure.Clinical trial registered with www.clinicaltrials.gov (NCT02503241).
Keywords: acute respiratory distress syndrome; hemodynamics; intrathoracic pressure; mechanical ventilation; obesity.
Figures
Comment in
-
Mechanical Ventilation in the Obese Patient: Compliance, Pleural Pressure, and Driving Pressure.Am J Respir Crit Care Med. 2021 Mar 1;203(5):534-536. doi: 10.1164/rccm.202009-3607ED. Am J Respir Crit Care Med. 2021. PMID: 32997946 Free PMC article. No abstract available.
-
Assessment of Airway Closure and Expiratory Airflow Limitation to Set Positive End-Expiratory Pressure in Morbidly Obese Patients with Acute Respiratory Distress Syndrome.Am J Respir Crit Care Med. 2021 Feb 1;203(3):391-392. doi: 10.1164/rccm.202009-3477LE. Am J Respir Crit Care Med. 2021. PMID: 33080139 Free PMC article. No abstract available.
-
Reply to Mezidi et al.: Assessment of Airway Closure and Expiratory Airflow Limitation to Set Positive End-Expiratory Pressure in Morbidly Obese Patients with Acute Respiratory Distress Syndrome.Am J Respir Crit Care Med. 2021 Feb 1;203(3):392-394. doi: 10.1164/rccm.202009-3641LE. Am J Respir Crit Care Med. 2021. PMID: 33080156 Free PMC article. No abstract available.
References
-
- Kolobow T, Moretti MP, Fumagalli R, Mascheroni D, Prato P, Chen V, et al. Severe impairment in lung function induced by high peak airway pressure during mechanical ventilation: an experimental study. Am Rev Respir Dis. 1987;135:312–315. - PubMed
-
- Pinsky MR. Heart-lung interactions during positive-pressure ventilation. New Horiz. 1994;2:443–456. - PubMed
-
- Mekontso Dessap A, Boissier F, Charron C, Bégot E, Repessé X, Legras A, et al. Acute cor pulmonale during protective ventilation for acute respiratory distress syndrome: prevalence, predictors, and clinical impact. Intensive Care Med. 2016;42:862–870. - PubMed
-
- Zapol WM, Snider MT. Pulmonary hypertension in severe acute respiratory failure. N Engl J Med. 1977;296:476–480. - PubMed
-
- Dreyfuss D, Basset G, Soler P, Saumon G. Intermittent positive-pressure hyperventilation with high inflation pressures produces pulmonary microvascular injury in rats. Am Rev Respir Dis. 1985;132:880–884. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
