

Coronary Angiography After Cardiac Arrest Without ST Segment Elevation: One-Year Outcomes of the COACT Randomized Clinical Trial
- PMID: 32876654
- PMCID: PMC7489423
- DOI: 10.1001/jamacardio.2020.3670
Coronary Angiography After Cardiac Arrest Without ST Segment Elevation: One-Year Outcomes of the COACT Randomized Clinical Trial
Abstract
Importance: Ischemic heart disease is a common cause of cardiac arrest. However, randomized data on long-term clinical outcomes of immediate coronary angiography and percutaneous coronary intervention (PCI) in patients successfully resuscitated from cardiac arrest in the absence of ST segment elevation myocardial infarction (STEMI) are lacking.
Objective: To determine whether immediate coronary angiography improves clinical outcomes at 1 year in patients after cardiac arrest without signs of STEMI, compared with a delayed coronary angiography strategy.
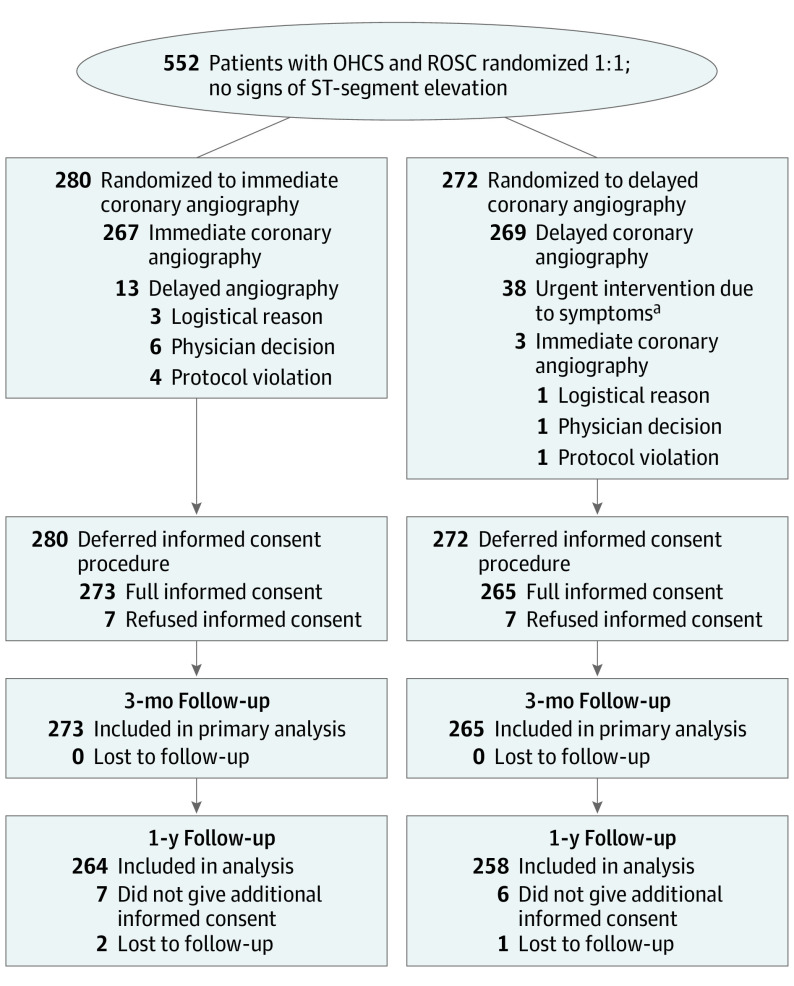
Design, setting, and participants: A prespecified analysis of a multicenter, open-label, randomized clinical trial evaluated 552 patients who were enrolled in 19 Dutch centers between January 8, 2015, and July 17, 2018. The study included patients who experienced out-of-hospital cardiac arrest with a shockable rhythm who were successfully resuscitated without signs of STEMI. Follow-up was performed at 1 year. Data were analyzed, using the intention-to-treat principle, between August 29 and October 10, 2019.
Interventions: Immediate coronary angiography and PCI if indicated or coronary angiography and PCI if indicated, delayed until after neurologic recovery.
Main outcomes and measures: Survival, myocardial infarction, revascularization, implantable cardiac defibrillator shock, quality of life, hospitalization for heart failure, and the composite of death or myocardial infarction or revascularization after 1 year.
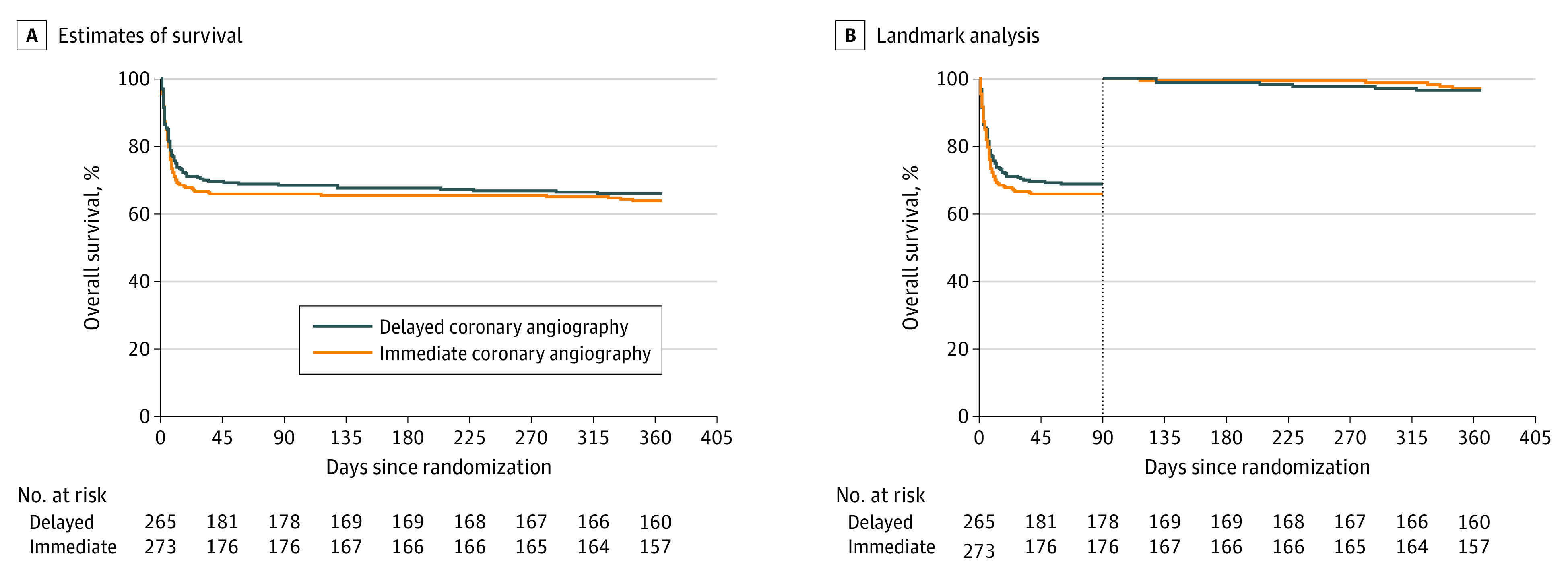
Results: At 1 year, data on 522 of 552 patients (94.6%) were available for analysis. Of these patients, 413 were men (79.1%); mean (SD) age was 65.4 (12.3) years. A total of 162 of 264 patients (61.4%) in the immediate angiography group and 165 of 258 patients (64.0%) in the delayed angiography group were alive (odds ratio, 0.90; 95% CI, 0.63-1.28). The composite end point of death, myocardial infarction, or repeated revascularization since the index hospitalization was met in 112 patients (42.9%) in the immediate group and 104 patients (40.6%) in the delayed group (odds ratio, 1.10; 95% CI, 0.77-1.56). No significant differences between the groups were observed for the other outcomes at 1-year follow-up. For example, the rate of ICD shocks was 20.4% in the immediate group and 16.2% in the delayed group (odds ratio, 1.32; 95% CI, 0.66-2.64).
Conclusions and relevance: In this trial of patients successfully resuscitated after out-of-hospital cardiac arrest and without signs of STEMI, a strategy of immediate angiography was not found to be superior to a strategy of delayed angiography with respect to clinical outcomes at 1 year. Coronary angiography in this patient group can therefore be delayed until after neurologic recovery without affecting outcomes.
Trial registration: trialregister.nl Identifier: NTR4973.
Conflict of interest statement
Figures
References
-
- Patel N, Patel NJ, Macon CJ, et al. . Trends and outcomes of coronary angiography and percutaneous coronary intervention after out-of-hospital cardiac arrest associated with ventricular fibrillation or pulseless ventricular tachycardia. JAMA Cardiol. 2016;1(8):890-899. doi:10.1001/jamacardio.2016.2860 - DOI - PubMed
-
- Ibanez B, James S, Agewall S, et al. . ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2017;2017. - PubMed
-
- O’Gara PT, Kushner FG, Ascheim DD, et al. . 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;61(4):e78-e140. doi:10.1016/j.jacc.2012.11.019 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Miscellaneous
