

Patient preferences for development in MRI scanner design: a survey of claustrophobic patients in a randomized study
- PMID: 32876831
- PMCID: PMC7880963
- DOI: 10.1007/s00330-020-07060-9
Patient preferences for development in MRI scanner design: a survey of claustrophobic patients in a randomized study
Abstract
Objective: To investigate which magnetic resonance imaging (MRI) scanner designs claustrophobic patients prefer.
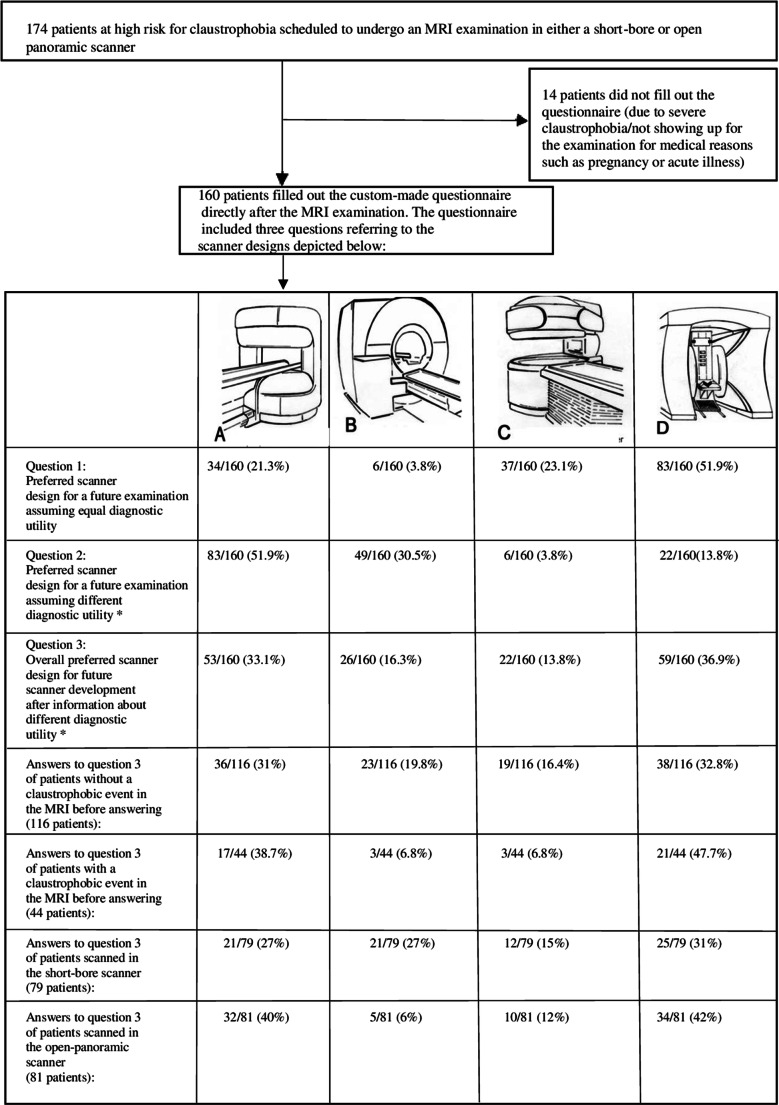
Material/methods: We analyzed questionnaires completed by 160 patients at high risk for claustrophobia directly after a scan in either a short-bore or open panoramic scanner as part of a prospective randomized trial Enders et al (BMC Med Imaging 11:4, 2011). Scanner preferences were judged based on schematic drawings of four scanners. Information on the diagnostic performance of the depicted scanners was provided, too.
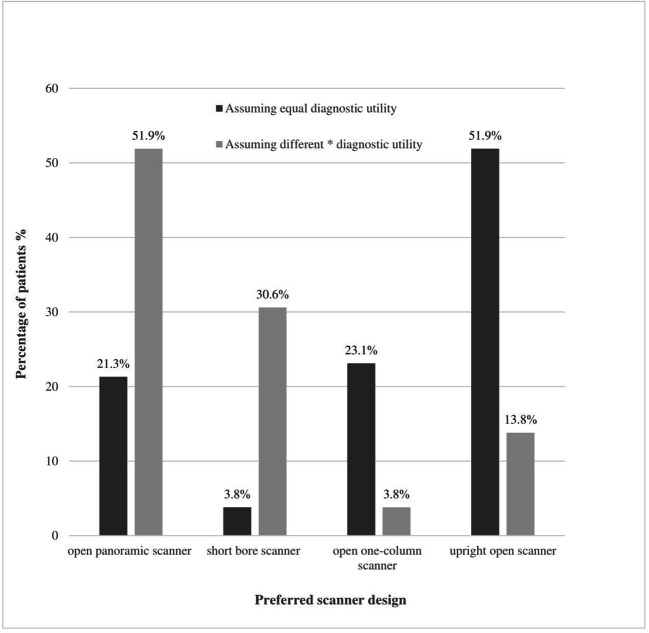
Results: A majority of patients suggested upright open (59/160, 36.9%) and open panoramic (53/160, 33.1%) before short-bore designs (26/160, 16.3%, for all p < 0.001) for future development. When asked about patients' preferred scanner choice for an upcoming examination, information about a better diagnostic performance of a short-bore scanner significantly improved its preference rates (from 6/160 to 49/160 or 3.8 to 30.5%, p < 0.001). Patients with a claustrophobic event preferred open designs significantly more often than patients without a claustrophobic event (p = 0.047). Patients scanned in a short-bore scanner in our trial preferred this design significantly more often (p = 0.003). Noise reduction (51/160, 31.9%), more space over the head (44/160, 27.5%), and overall more space (33/160, 20.6%) were the commonest suggested areas of improvement.
Conclusion: Patients at high risk for claustrophobia visually prefer open- over short-bore MRI designs for further development. Education about a better diagnostic performance of a visually less-attractive scanner can increase its acceptance. Noise and space were of most concern for claustrophobic patients. This information can guide individual referral of claustrophobic patients to scanners and future scanner development.
Key points: • Patients at high risk for claustrophobia visually favor the further development of open scanners as opposed to short- and closed-bore scanner designs. • Educating claustrophobic patients about a higher diagnostic performance of a short-bore scanner can significantly increase their acceptance of this otherwise visually less-attractive design. • A medical history of earlier claustrophobic events in a given MRI scanner type and focusing on the features "more space" and "noise reduction" can help to guide referral of patients who are at high risk for claustrophobia.
Keywords: Claustrophobia; Magnetic resonance imaging; Questionnaire.
Conflict of interest statement
The authors of this manuscript declare relationships with the following companies:
Prof. Dewey has received grant support from the FP7 Program of the European Commission for the randomized multicenter DISCHARGE trial (603266-2, HEALTH-2012.2.4.-2). He also received grant support from German Research Foundation (DFG) in the Heisenberg Program (DE 1361/14-1), graduate program on quantitative biomedical imaging (BIOQIC, GRK 2260/1), for fractal analysis of myocardial perfusion (DE 1361/18-1), and the Priority Programme Radiomics for the investigation of coronary plaque and coronary flow (DE 1361/19-1 (428222922) and 20-1 (428223139) in SPP 2177/1). He also received funding from the Berlin University Alliance (GC_SC_PC 27) and from the Digital Health Accelerator of the Berlin Institute of Health. Prof. Dewey has received lecture fees from Canon, Guerbet. Prof. Dewey is the European Society of Radiology (ESR) Research Chair (2019–2022) and the opinions expressed in this article are the author’s own and do not represent the view of ESR. Per the guiding principles of ESR, the work as Research Chair is on a voluntary basis and only remuneration of travel expenses occurs. Prof. Dewey is also the editor of
The other authors reported no financial disclosures for this article.
Figures




References
-
- Rachman S, Taylor S. Analyses of claustrophobia. J Anxiety Disord. 1993;7(4):281–291. doi: 10.1016/0887-6185(93)90025-G. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
