

Neurological injuries in COVID-19 patients: direct viral invasion or a bystander injury after infection of epithelial/endothelial cells
- PMID: 32876900
- PMCID: PMC7465881
- DOI: 10.1007/s13365-020-00903-7
Neurological injuries in COVID-19 patients: direct viral invasion or a bystander injury after infection of epithelial/endothelial cells
Abstract
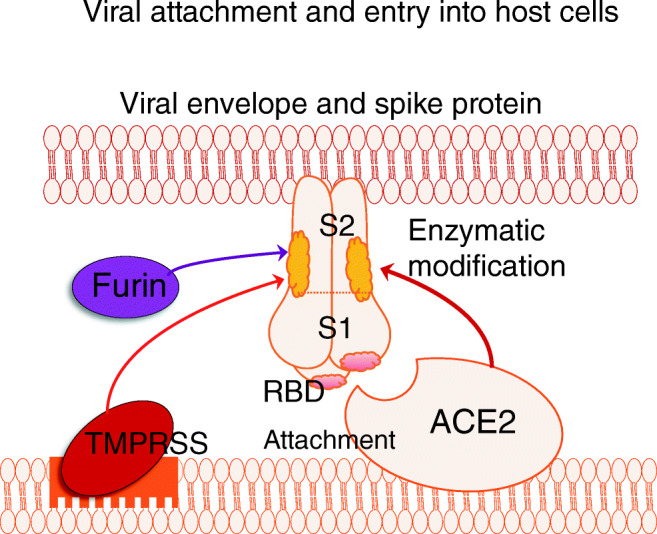
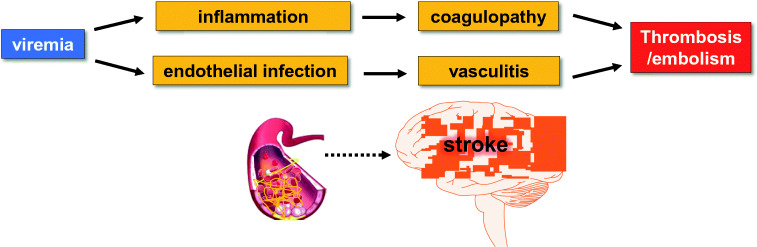
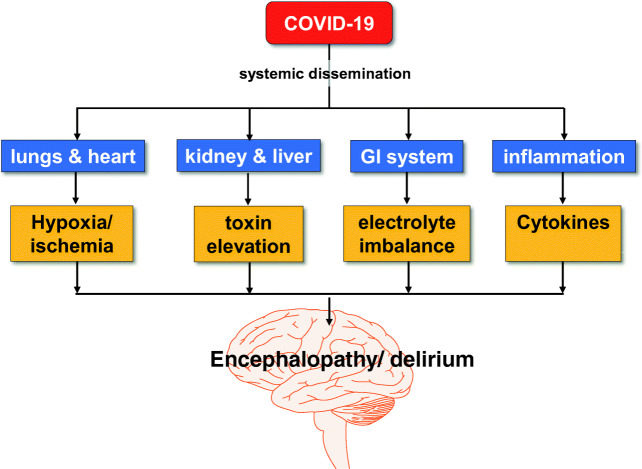
A subset of patients with coronavirus 2 disease (COVID-19) experience neurological complications. These complications include loss of sense of taste and smell, stroke, delirium, and neuromuscular signs and symptoms. The etiological agent of COVID-19 is SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2), an RNA virus with a glycoprotein-studded viral envelope that uses ACE2 (angiotensin-converting enzyme 2) as a functional receptor for infecting the host cells. Thus, the interaction of the envelope spike proteins with ACE2 on host cells determines the tropism and virulence of SARS-CoV-2. Loss of sense of taste and smell is an initial symptom of COVID-19 because the virus enters the nasal and oral cavities first and the epithelial cells are the receptors for these senses. Stroke in COVID-19 patients is likely a consequence of coagulopathy and injury to cerebral vascular endothelial cells that cause thrombo-embolism and stroke. Delirium and encephalopathy in acute and post COVID-19 patients are likely multifactorial and secondary to hypoxia, metabolic abnormalities, and immunological abnormalities. Thus far, there is no clear evidence that coronaviruses cause inflammatory neuromuscular diseases via direct invasion of peripheral nerves or muscles or via molecular mimicry. It appears that most of neurologic complications in COVID-19 patients are indirect and as a result of a bystander injury to neurons.
Keywords: ACE2; COVID-19; Encephalopathy; SARS-CoV-2; Smell; Stroke; Taste; Tropism.
Figures

References
-
- Ackermann M, Verlenden SE, Kuehnel M, Haverich A, Welte T, Laenger F, Vanstaplel A, Werlein C, Stark H, Zakov A, Li WW, Li VW, Mentzger SJ, Jonigk D. Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in COVID-19. NEJM. 2020;383:120–128. doi: 10.1056/NEJMoa2015432. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
