

Optimizing therapy in the modern age: differences in length of maintenance therapy in acute lymphoblastic leukemia
- PMID: 32877503
- PMCID: PMC7820874
- DOI: 10.1182/blood.2020007702
Optimizing therapy in the modern age: differences in length of maintenance therapy in acute lymphoblastic leukemia
Abstract
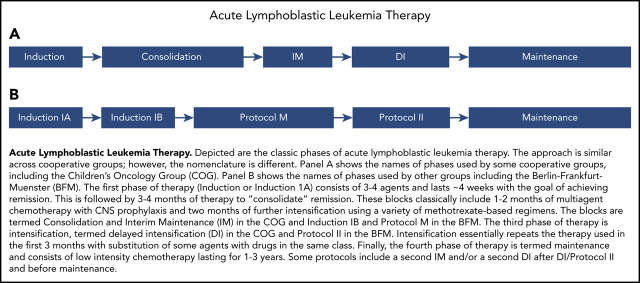
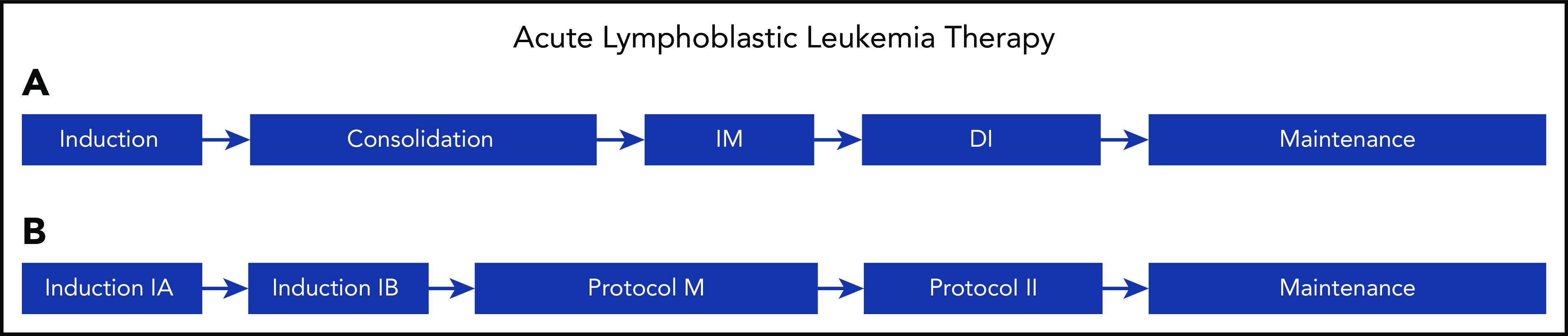
A majority of children and young adults with acute lymphoblastic leukemia (ALL) are cured with contemporary multiagent chemotherapy regimens. The high rate of survival is largely the result of 70 years of randomized clinical trials performed by international cooperative groups. Contemporary ALL therapy usually consists of cycles of multiagent chemotherapy administered over 2 to 3 years that includes central nervous system (CNS) prophylaxis, primarily consisting of CNS-penetrating systemic agents and intrathecal therapy. Although the treatment backbones vary among cooperative groups, the same agents are used, and the outcomes are comparable. ALL therapy typically begins with 5 to 9 months of more-intensive chemotherapy followed by a prolonged low-intensity maintenance phase. Historically, a few cooperative groups treated boys with 1 more year of maintenance therapy than girls; however, most groups treated boys and girls with equal therapy lengths. This practice arose because of inferior survival in boys with older less-intensive regimens. The extra year of therapy added significant burden to patients and families and involved short- and long-term risks that were potentially life threatening and debilitating. The Children's Oncology Group recently changed its approach as part of its current generation of trials in B-cell ALL and now treats boys and girls with the same duration of therapy. We discuss the rationale behind this change, review the data and differences in practice across cooperative groups, and provide our perspective regarding the length of maintenance therapy.
© 2021 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: D.T.T. serves on advisory boards for Janssen, Amgen, La Roche, Sobi, and Humanigen. S.P.H. owns stock in Amgen and has received consulting fees from Novartis and honoraria from Amgen. M.L.L. serves on the advisory board for MediSix Therapeutics.
Figures
References
-
- Simone JV History of the treatment of childhood ALL: a paradigm for cancer cure. Best Pract Res Clin Haematol. 2006;19(2):353-359. - PubMed
-
- Farber S, Diamond LK. Temporary remissions in acute leukemia in children produced by folic acid antagonist, 4-aminopteroyl-glutamic acid. N Engl J Med. 1948;238(23):787-793. - PubMed
-
- Elion GB, Bieber S, Hitchings GH. A summary of investigations with 2-amino-6-[(1-methyl-4-nitro-5-imidazolyl)thio]purine (B.W. 57-323) in animals. Cancer Chemother Rep. 1960;8:36-43. - PubMed
-
- Pinkel D Therapy of acute lymphoid leukemia in children. Leukemia. 1992;6(suppl 2):127-131. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
