

Sleep and its regulation: An emerging pathogenic and treatment frontier in Alzheimer's disease
- PMID: 32877742
- PMCID: PMC7855222
- DOI: 10.1016/j.pneurobio.2020.101902
Sleep and its regulation: An emerging pathogenic and treatment frontier in Alzheimer's disease
Abstract
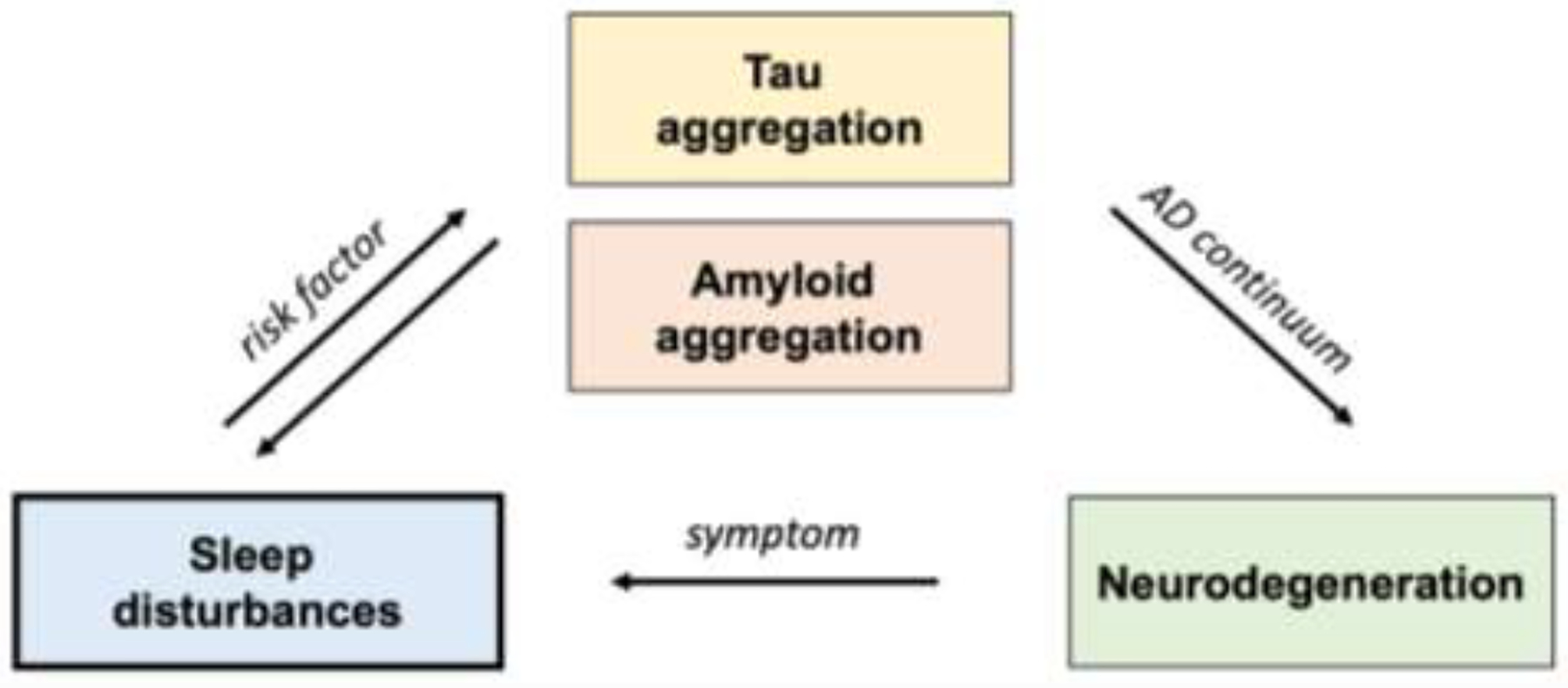
A majority of patients with Alzheimer's disease (AD) experience some form of sleep disruption, including nocturnal sleep fragmentation, increased daytime napping, decreased slow-wave sleep (SWS, stage N3), and decreased rapid-eye-movement sleep (REM). Clinical studies are investigating whether such sleep disturbances are a consequence of the underlying disease, and whether they also contribute to the clinical and pathological manifestations of AD. Emerging research has provided a direct link between several of these sleep disruptions and AD pathophysiology, suggesting that treating sleep disorders in this population may target basic mechanisms of the disease. Here, we provide a comprehensive review of sleep disturbances associated with the spectrum of AD, ranging from the preclinical stages through dementia. We discuss how sleep interacts with AD pathophysiology and, critically, whether sleep impairments can be targeted to modify the disease course in a subgroup of affected AD patients. Ultimately, larger studies that fully utilize new diagnostic and experimental tools will be required to better define the most relevant sleep disturbance to target in AD, the interventions that best modulate this target symptom, and whether successful early intervention can modify AD risk and prevent dementia.
Keywords: Alzheimer’s disease; Circadian rhythms; Dementia; EEG; Power spectra; Sleep.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Figures


References
-
- Adler G, & Brassen S, 2001. Short-term rivastigmine treatment reduces EEG slow-wave power in Alzheimer patients. Neuropsychobiology 43, 273–276. - PubMed
-
- Ancoli-Israel S, Klauber MR, Gillin JC, Campbell SS, & Hofstetter CR, 1994. Sleep in non-institutionalized Alzheimer’s disease patients. Aging Clinical and Experimental Research 6, 451–458. - PubMed
-
- Arendt J, Skene DJ, Middleton B, Lockley SW, Deacon S, 1997. Efficacy of melatonin treatment in jet lag, shift work, and blindness. Journal of biological rhythms 12, 604–617. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
