

Evaluation of Multi-Layered Pancreatic Islets and Adipose-Derived Stem Cell Sheets Transplanted on Various Sites for Diabetes Treatment
- PMID: 32878048
- PMCID: PMC7563383
- DOI: 10.3390/cells9091999
Evaluation of Multi-Layered Pancreatic Islets and Adipose-Derived Stem Cell Sheets Transplanted on Various Sites for Diabetes Treatment
Abstract
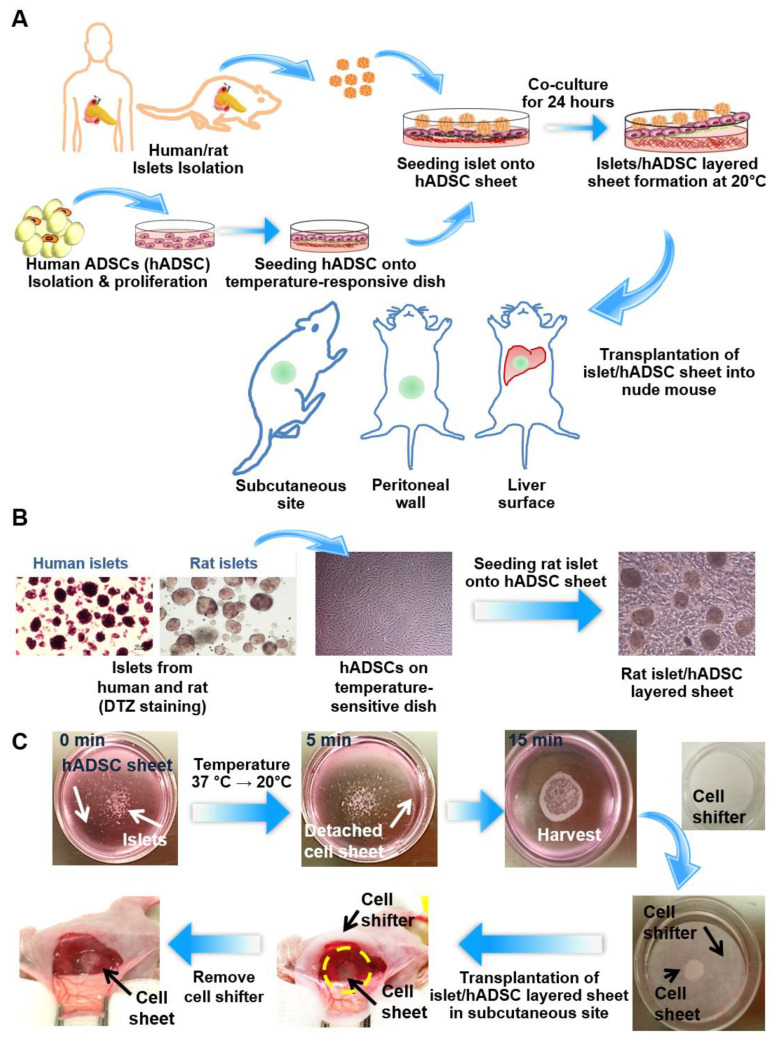
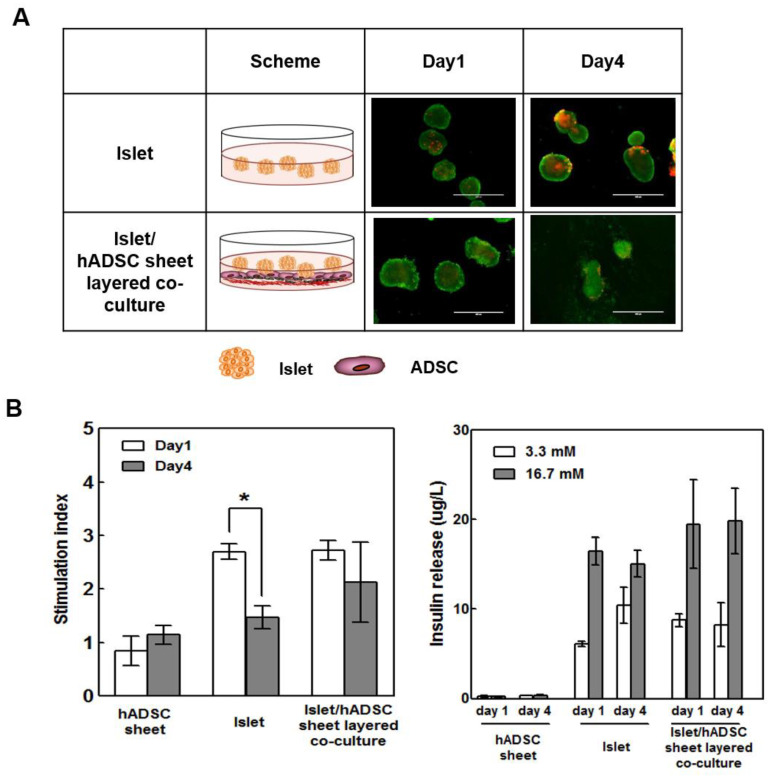
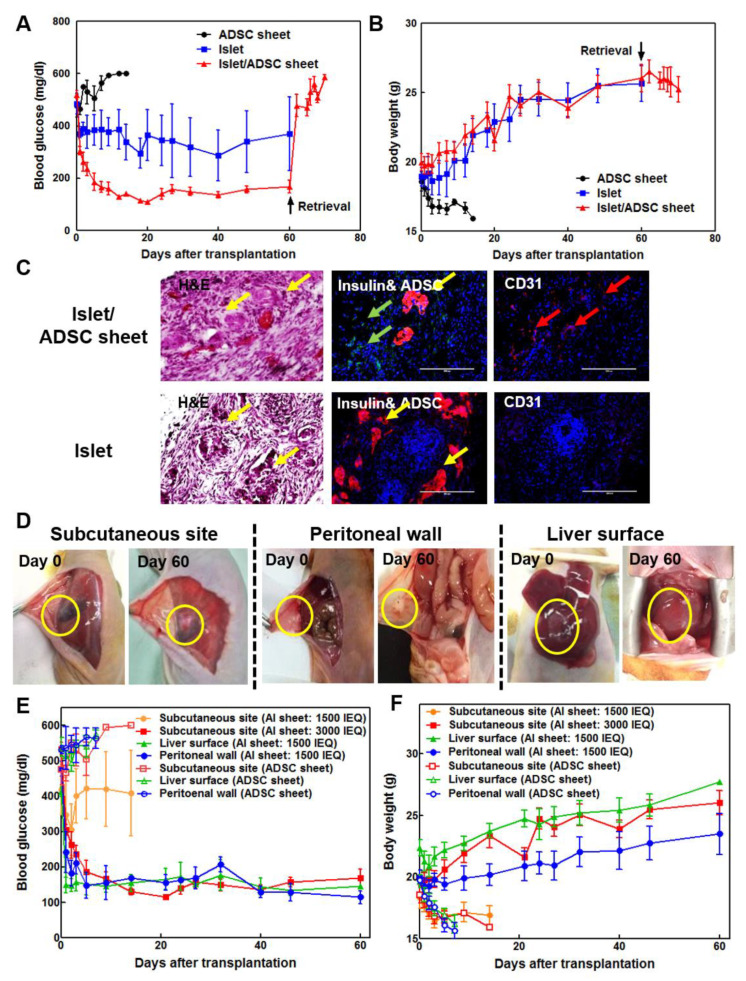
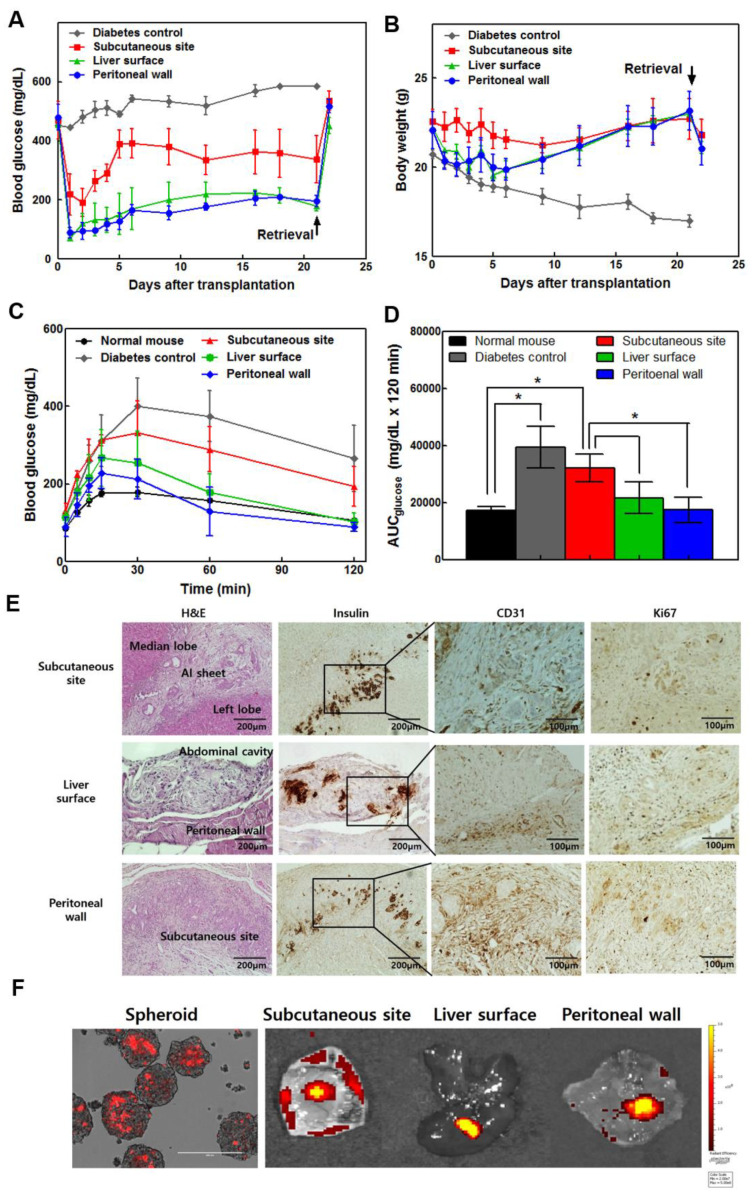
Islet cell transplantation is considered an ideal treatment for insulin-deficient diabetes, but implantation sites are limited and show low graft survival. Cell sheet technology and adipose-derived stem cells (ADSCs) can be useful tools for improving islet cell transplantation outcomes since both can increase implantation efficacy and graft survival. Herein, the optimal transplantation site in diabetic mice was investigated using islets and stem cell sheets. We constructed multi-layered cell sheets using rat/human islets and human ADSCs. Cell sheets were fabricated using temperature-responsive culture dishes. Islet/ADSC sheet (AI sheet) group showed higher viability and glucose-stimulated insulin secretion than islet-only group. Compared to islet transplantation alone, subcutaneous AI sheet transplantation showed better blood glucose control and CD31+ vascular traits. Because of the adhesive properties of cell sheets, AI sheets were easily applied on liver and peritoneal surfaces. Liver or peritoneal surface grafts showed better glucose control, weight gain, and intraperitoneal glucose tolerance test (IPGTT) profiles than subcutaneous site grafts using both rat and human islets. Stem cell sheets increased the therapeutic efficacy of islets in vivo because mesenchymal stem cells enhance islet function and induce neovascularization around transplanted islets. The liver and peritoneal surface can be used more effectively than the subcutaneous site in future clinical applications.
Keywords: adipose-derived stem cell; islet; liver surface; multi-layered cell sheet; peritoneal wall; subcutaneous site; transplantation.
Conflict of interest statement
Teruo Okano is a founder and director of the Scientific Advisory Board of CellSeed Inc., which has licenses for certain cell sheet-related technologies and patents from Tokyo Women’s Medical University. Yu Na Lee, Hye-Jin Yi, Yang Hee Kim, Song Lee, Jooyun Oh, In Kyong Shim, and Song Cheol Kim declare no potential conflict of interest. The authors declare that there are no other financial or non-financial competing interests. The authors of the article do not have any commercial association (e.g., consultancies, stock ownership, equity interests, or patent-licensing arrangements) that might pose a conflict of interest in connection with the submitted article.
Figures
References
-
- Ichii H., Inverardi L., Pileggi A., Molano R.D., Cabrera O., Caicedo A., Messinger S., Kuroda Y., Berggren P.-O., Ricordi C. A novel method for the assessment of cellular composition and beta-cell viability in human islet preparations. Am. J. Transplant. 2005;5:1635–1645. doi: 10.1111/j.1600-6143.2005.00913.x. - DOI - PubMed
-
- Contreras J.L., Eckstein C., Smyth C.A., Bilbao G., Vilatoba M., Ringland S.E., Young C., Thompson J.A., Fernández J.A., Griffin J.H., et al. Activated protein C preserves functional islet mass after intraportal transplantation: A novel link between endothelial cell activation, thrombosis, inflammation, and islet cell death. Diabetes. 2004;53:2804–2814. doi: 10.2337/diabetes.53.11.2804. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
