

Management of Non-Tubal Ectopic Pregnancies: A Single Center Experience
- PMID: 32878097
- PMCID: PMC7555978
- DOI: 10.3390/diagnostics10090652
Management of Non-Tubal Ectopic Pregnancies: A Single Center Experience
Abstract
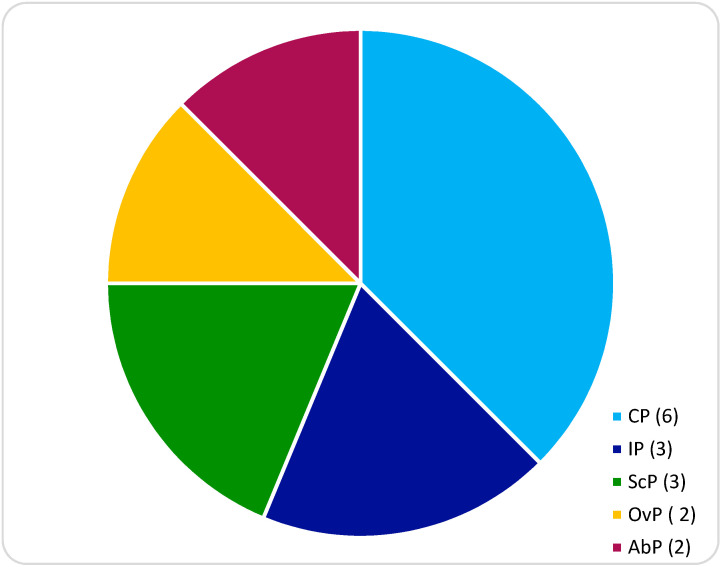
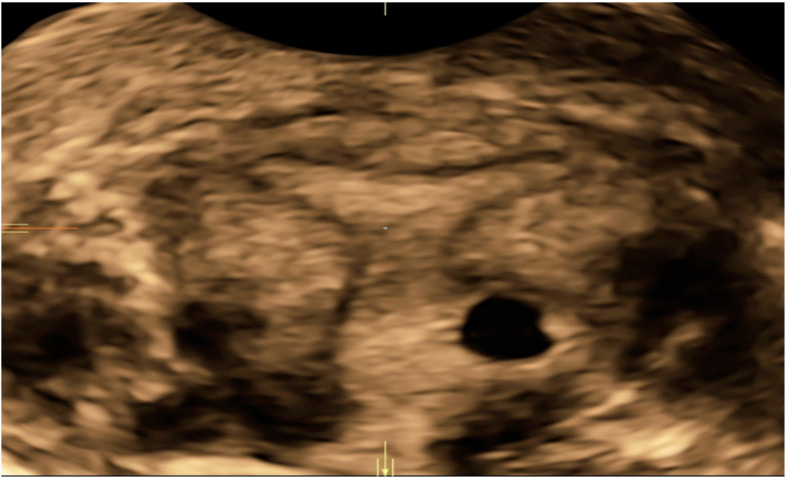
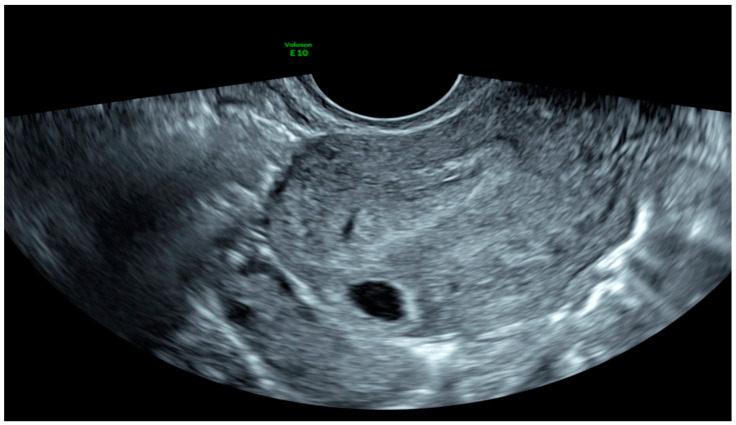
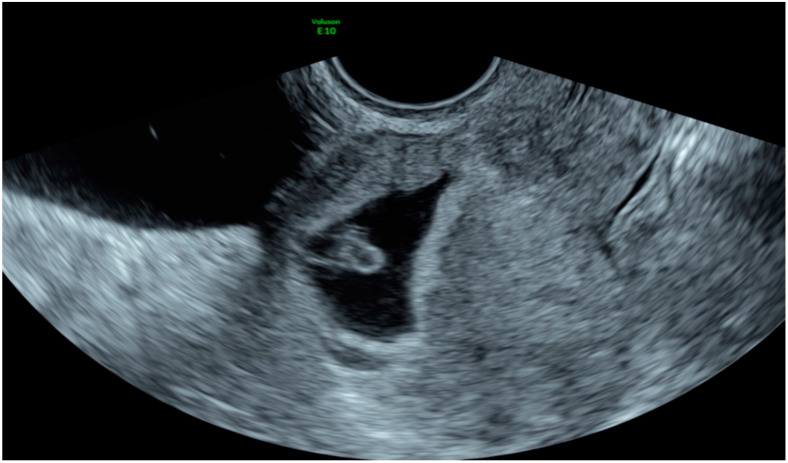
Non-tubal ectopic pregnancies (NT-EPs) are rare but potentially life-threatening conditions. The incidence ranges are between 5-8.3% of all ectopic pregnancies. For this retrospective observational study, 16 patients with NT-EP and treated from January 2014 to May 2020 were recruited. Demographic details, symptoms, Beta human chorionic gonadotrophin (β-hCG) levels, ultrasound findings, management and treatment outcomes were presented. In hemodynamically stable patients, diagnosis was made using ultrasounds and β-hCG levels. Laparoscopy was essential to identify and remove the ectopic pregnancy in clinical unstable patients. A radical laparoscopic approach was chosen in one case of cervical pregnancy diagnosed late in the first trimester. Medical treatment and minimally invasive procedure, alone or combined, resulted in effective strategies in asymptomatic women with an early diagnosis of NT-EP. We report cases of cervical pregnancies successfully treated by hysteroscopy alone or combined with medical treatment, the first case of scar pregnancy treated by mini-reseptoscope and curettage and the fifth case of interstitial pregnancy treated with Methotrexate and Mifepristone. In this manuscript we report a single center experience in the management of NT-EPs with the aim of outlining the importance of the early diagnosis for a minimally invasive treatment in order to reduce maternal morbidity and mortality and preserve future fertility.
Keywords: ectopic non-tubal pregnancy; fertility sparing; hysteroscopy; laparoscopy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Prameela R., Dev S. Cervical ectopic pregnancy: 10 year experience at tertiary care hospital and current literature review. Int. J. Reprod. Contracept. Obstet. Gynecol. 2016 doi: 10.18203/2320-1770.ijrcog20160575. - DOI
LinkOut - more resources
Full Text Sources
Research Materials
