

Towards more efficient use of intravenous lumens in multi-infusion settings: development and evaluation of a multiplex infusion scheduling algorithm
- PMID: 32878609
- PMCID: PMC7466776
- DOI: 10.1186/s12911-020-01231-w
Towards more efficient use of intravenous lumens in multi-infusion settings: development and evaluation of a multiplex infusion scheduling algorithm
Abstract
Background: Multi-drug intravenous (IV) therapy is one of the most common medical procedures used in intensive care units (ICUs), operating rooms, oncology wards and many other hospital departments worldwide. As drugs or their solvents are frequently chemically incompatible, many solutions must be administered through separate lumens. When the number of available lumens is too low to facilitate the safe administration of these solutions, additional (peripheral) IV catheters are often required, causing physical discomfort and increasing the risk for catheter related complications. Our objective was to develop and evaluate an algorithm designed to reduce the number of intravenous lumens required in multi-infusion settings by multiplexing the administration of various parenteral drugs and solutions.
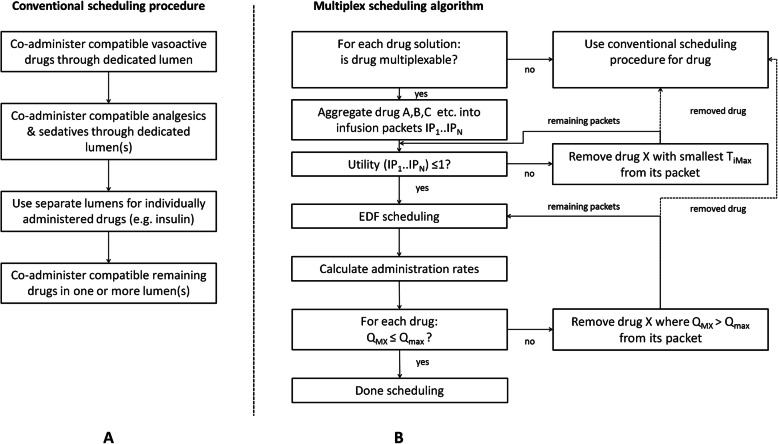
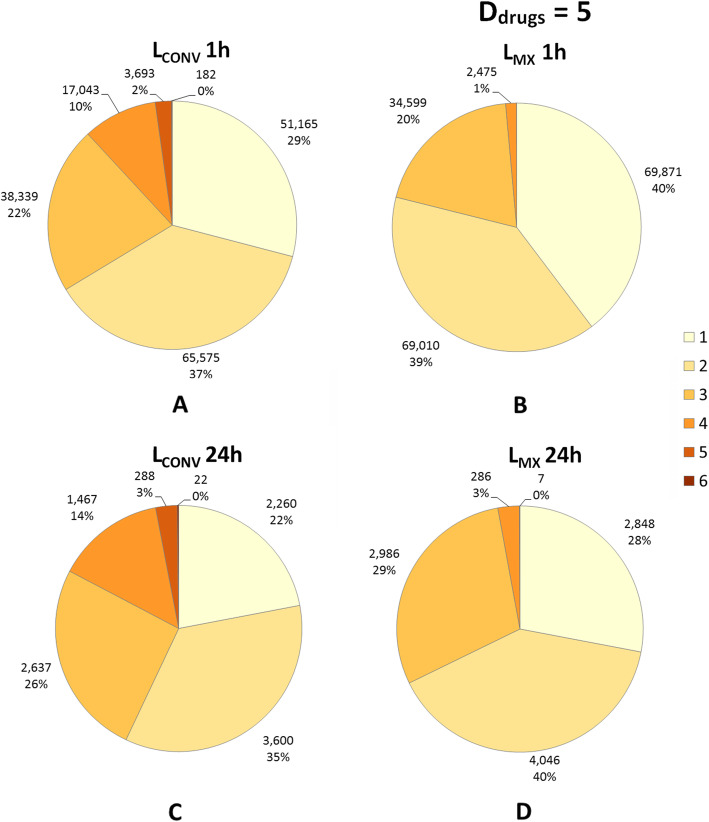
Methods: A multiplex algorithm was developed that schedules the alternating IV administration of multiple incompatible IV solutions through a single lumen, taking compatibility-related, pharmacokinetic and pharmacodynamic constraints of the relevant drugs into account. The conventional scheduling procedure executed by ICU nurses was used for comparison. The number of lumens required by the conventional procedure (LCONV) and multiplex algorithm (LMX) were compared.
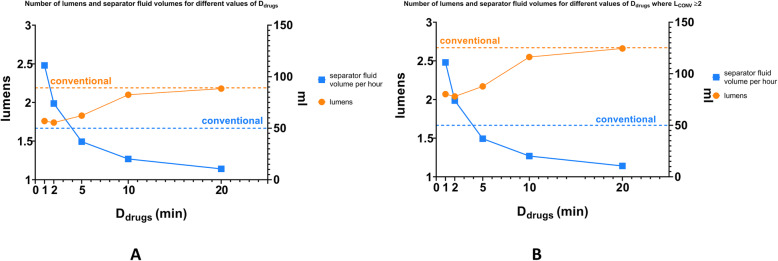
Results: We used data from 175,993 ICU drug combinations, with 2251 unique combinations received by 2715 consecutive ICU patients. The mean ± SD number of simultaneous IV solutions was 2.8 ± 1.6. In 27% of all drug combinations, and 61% of the unique combinations the multiplex algorithm required fewer lumens (p < 0.001). With increasing LCONV, the reduction in number of lumens by the multiplex algorithm further increased (p < 0.001). In only 1% of cases multiplexing required > 3 lm, versus 12% using the conventional procedure.
Conclusion: The multiplex algorithm addresses a major issue that occurs in ICUs, operating rooms, oncology wards, and many other hospital departments where several incompatible drugs are infused through a restricted number of lumens. The multiplex algorithm allows for more efficient use of IV lumens compared to the conventional multi-infusion strategy.
Keywords: Algorithms; Drug incompatibility; Infusion pumps; Infusions, intravenous; Injection site reaction.
Conflict of interest statement
Frank Doesburg and Maarten Nijsten are credited as co-inventors on a patent “System for providing multiple infusions to a patient” that was filed by Fresenius Kabi. Fresenius Kabi had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
