

COVID-19 length of hospital stay: a systematic review and data synthesis
- PMID: 32878619
- PMCID: PMC7467845
- DOI: 10.1186/s12916-020-01726-3
COVID-19 length of hospital stay: a systematic review and data synthesis
Abstract
Background: The COVID-19 pandemic has placed an unprecedented strain on health systems, with rapidly increasing demand for healthcare in hospitals and intensive care units (ICUs) worldwide. As the pandemic escalates, determining the resulting needs for healthcare resources (beds, staff, equipment) has become a key priority for many countries. Projecting future demand requires estimates of how long patients with COVID-19 need different levels of hospital care.
Methods: We performed a systematic review of early evidence on length of stay (LoS) of patients with COVID-19 in hospital and in ICU. We subsequently developed a method to generate LoS distributions which combines summary statistics reported in multiple studies, accounting for differences in sample sizes. Applying this approach, we provide distributions for total hospital and ICU LoS from studies in China and elsewhere, for use by the community.
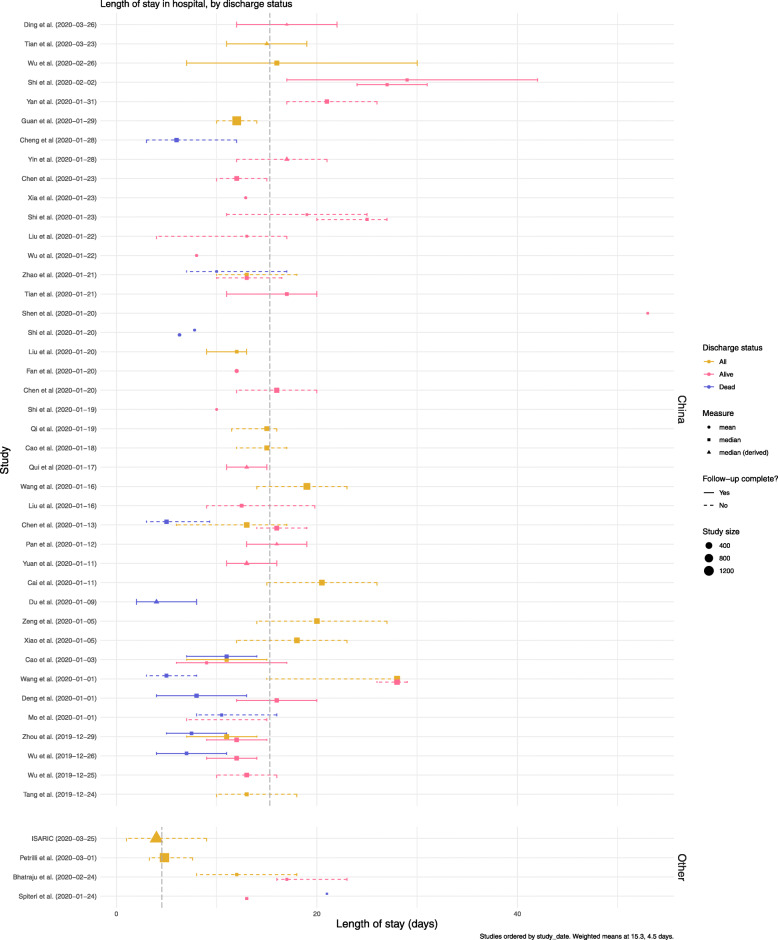
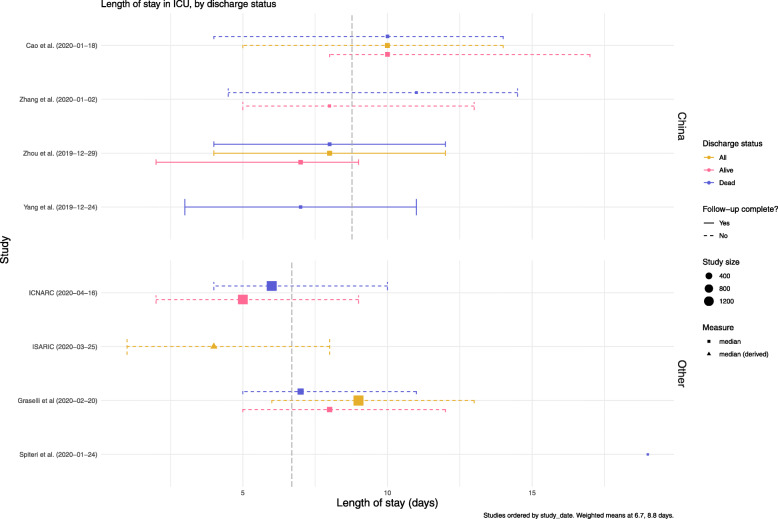
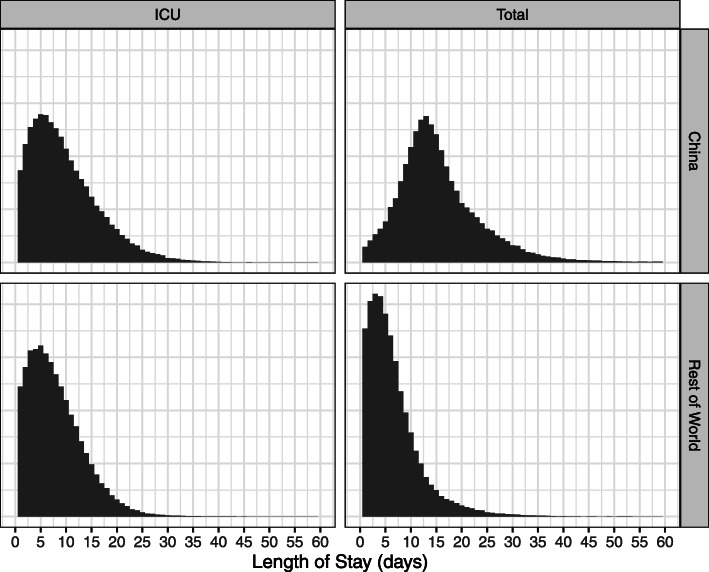
Results: We identified 52 studies, the majority from China (46/52). Median hospital LoS ranged from 4 to 53 days within China, and 4 to 21 days outside of China, across 45 studies. ICU LoS was reported by eight studies-four each within and outside China-with median values ranging from 6 to 12 and 4 to 19 days, respectively. Our summary distributions have a median hospital LoS of 14 (IQR 10-19) days for China, compared with 5 (IQR 3-9) days outside of China. For ICU, the summary distributions are more similar (median (IQR) of 8 (5-13) days for China and 7 (4-11) days outside of China). There was a visible difference by discharge status, with patients who were discharged alive having longer LoS than those who died during their admission, but no trend associated with study date.
Conclusion: Patients with COVID-19 in China appeared to remain in hospital for longer than elsewhere. This may be explained by differences in criteria for admission and discharge between countries, and different timing within the pandemic. In the absence of local data, the combined summary LoS distributions provided here can be used to model bed demands for contingency planning and then updated, with the novel method presented here, as more studies with aggregated statistics emerge outside China.
Keywords: Bed demand; COVID-19; Hospitalisation; ICU capacity; Length of stay; SARS-CoV-2.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- World Health Organization. Coronavirus disease 2019 (COVID-19) situation report, 95. 2020. Available from: https://www.who.int/docs/defaultsource/coronaviruse/situation-reports/20...\_4.
-
- Remuzzi A, Remuzzi G. COVID-19 and Italy: what next?Lancet. 2020; 395(10231):1225–8. Available from: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)3062%.... - PMC - PubMed
-
- Paterlini M. On the front lines of coronavirus: the Italian response to covid-19. BMJ. 2020; 368:m1065. Available from: https://www.bmj.com/content/368/bmj.m1065. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
