

Association of genetic risk for Alzheimer disease and hearing impairment
- PMID: 32878991
- PMCID: PMC7713783
- DOI: 10.1212/WNL.0000000000010709
Association of genetic risk for Alzheimer disease and hearing impairment
Abstract
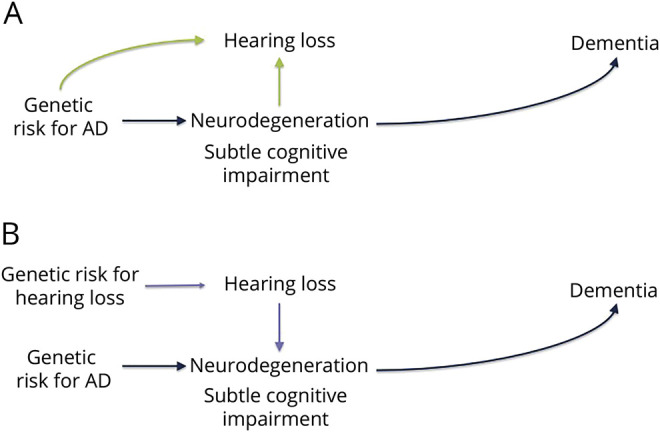
Objective: To test the hypothesis that incipient Alzheimer disease (AD) may adversely affect hearing and that hearing loss may adversely affect cognition, we evaluated whether genetic variants that increase AD risk also increase problem hearing and genetic variants that increase hearing impairment risk do not influence cognition.
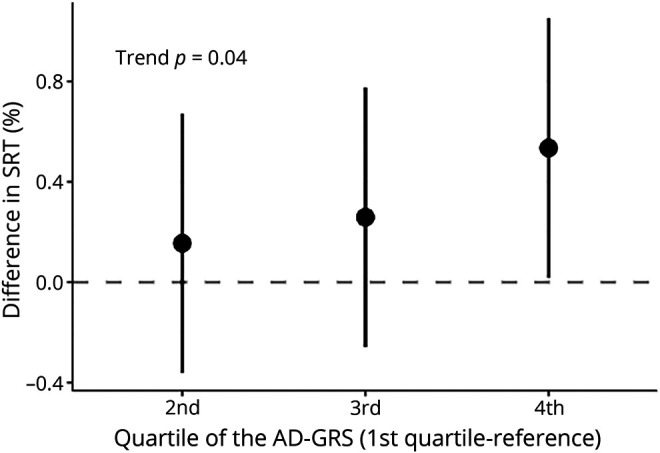
Methods: UK Biobank participants without dementia ≥56 years of age with Caucasian genetic ancestry completed a Digit Triplets Test of speech-in-noise hearing (n = 80,074), self-reported problem hearing and hearing with background noise (n = 244,915), and completed brief cognitive assessments. A genetic risk score for AD (AD-GRS) was calculated as a weighted sum of 23 previously identified AD-related polymorphisms. A genetic risk score for hearing (hearing-GRS) was calculated using 3 previously identified polymorphisms related to hearing impairment. Using age-, sex-, and genetic ancestry-adjusted logistic and linear regression models, we evaluated whether the AD-GRS predicted poor hearing and whether the hearing-GRS predicted worse cognition.
Results: Poor speech-in-noise hearing (>-5.5-dB speech reception threshold; prevalence 14%) was associated with lower cognitive scores (ß = -1.28; 95% confidence interval [CI] -1.54 to -1.03). Higher AD-GRS was significantly associated with poor speech-in-noise hearing (odds ratio [OR] 1.06; 95% CI 1.01-1.11) and self-reported problems hearing with background noise (OR 1.03; 95% CI 1.00-1.05). Hearing-GRS was not significantly associated with cognitive scores (ß = -0.05; 95% CI -0.17 to 0.07).
Conclusions: Genetic risk for AD also influences speech-in-noise hearing. We failed to find evidence that genetic risk for hearing impairment affects cognition. AD disease processes or a that shared etiology may cause speech-in-noise difficulty before dementia onset.
© 2020 American Academy of Neurology.
Figures
References
-
- Livingston G, Sommerlad A, Orgeta V, et al. Dementia prevention, intervention, and care. Lancet. 2017;390:2673–2734. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous