

Sacropelvic fixation techniques - Current update
- PMID: 32879572
- PMCID: PMC7452281
- DOI: 10.1016/j.jcot.2020.07.022
Sacropelvic fixation techniques - Current update
Erratum in
-
Erratum regarding previously published articles.J Clin Orthop Trauma. 2021 Aug 5;21:101558. doi: 10.1016/j.jcot.2021.101558. eCollection 2021 Oct. J Clin Orthop Trauma. 2021. PMID: 34414072 Free PMC article.
Abstract
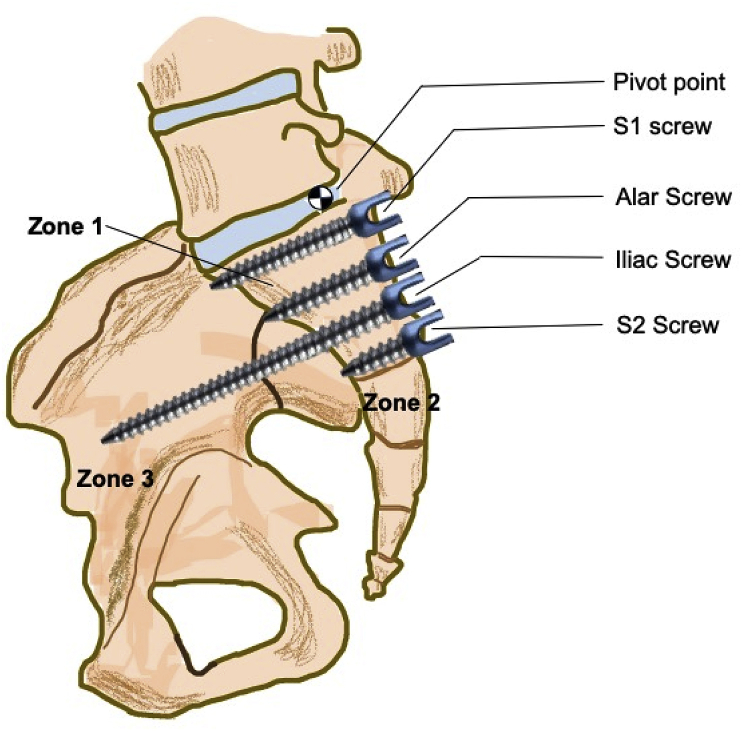
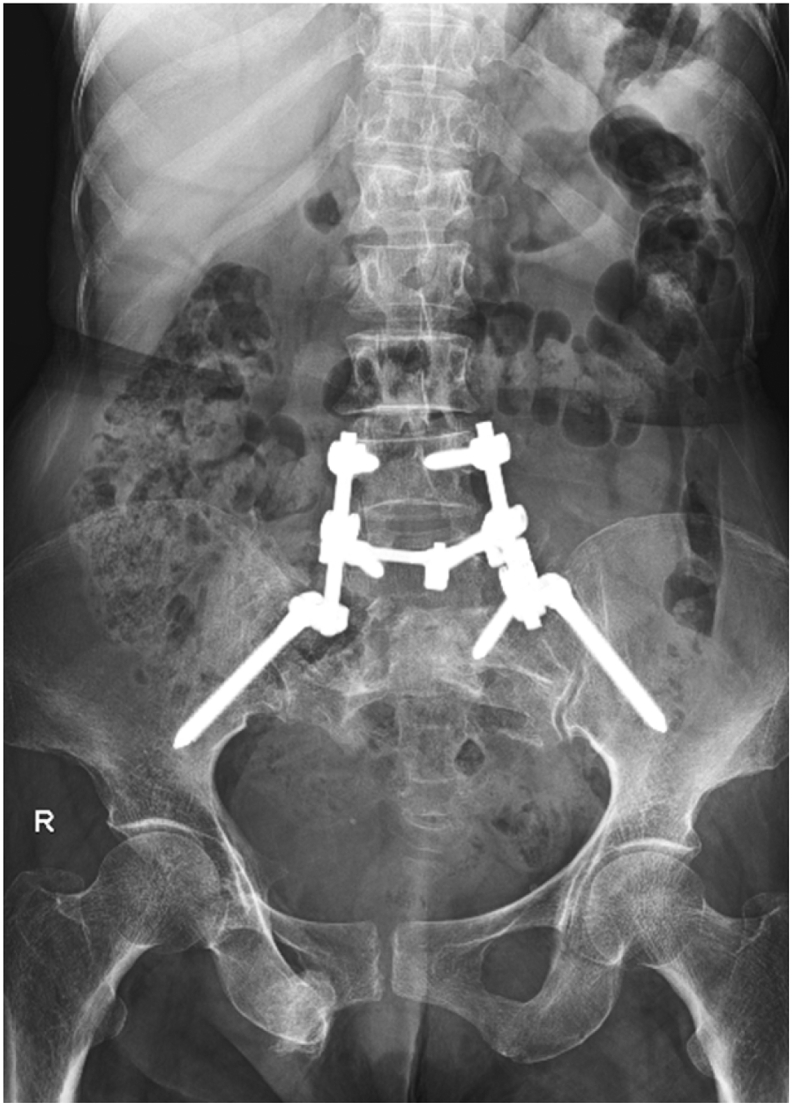
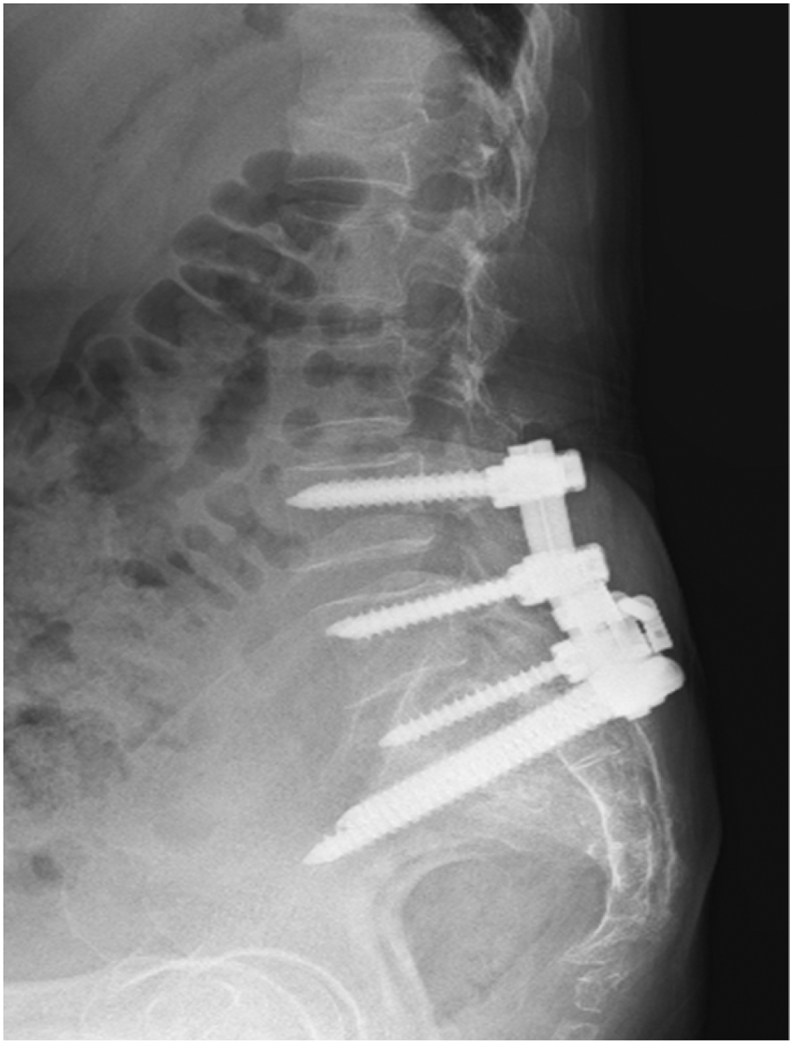
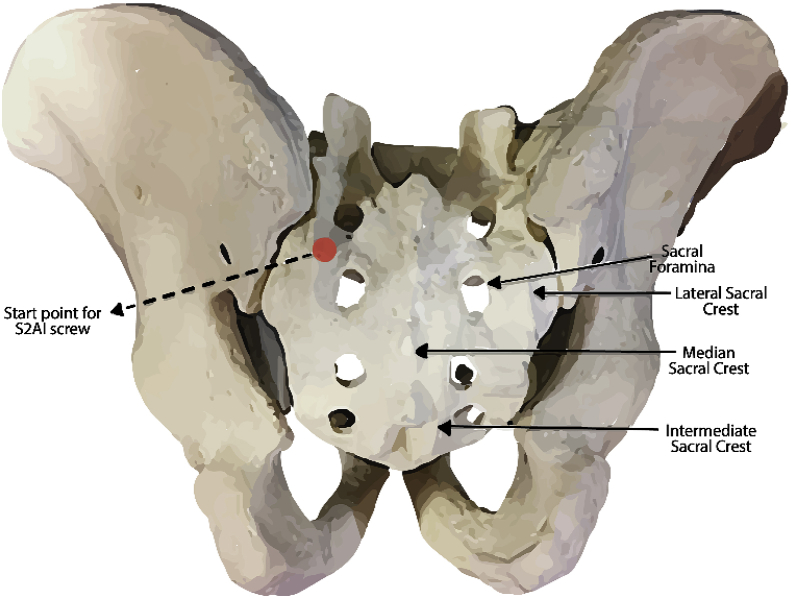
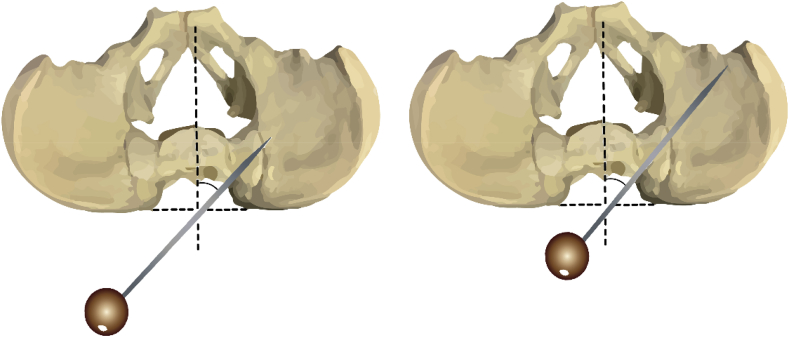
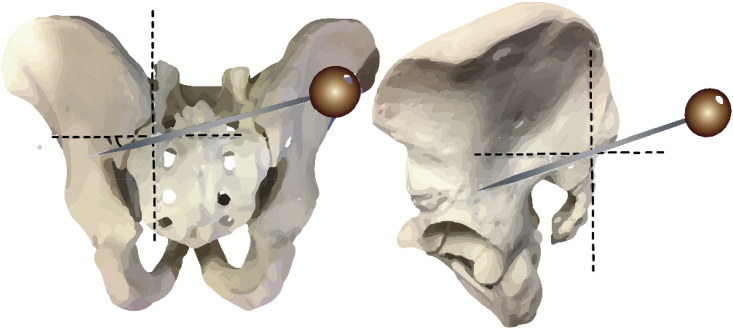
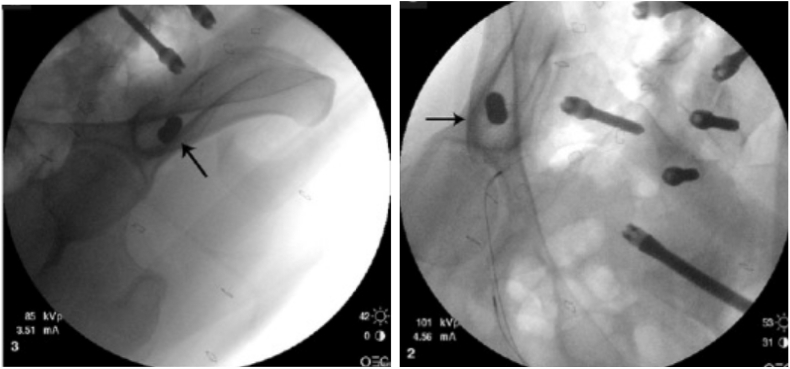
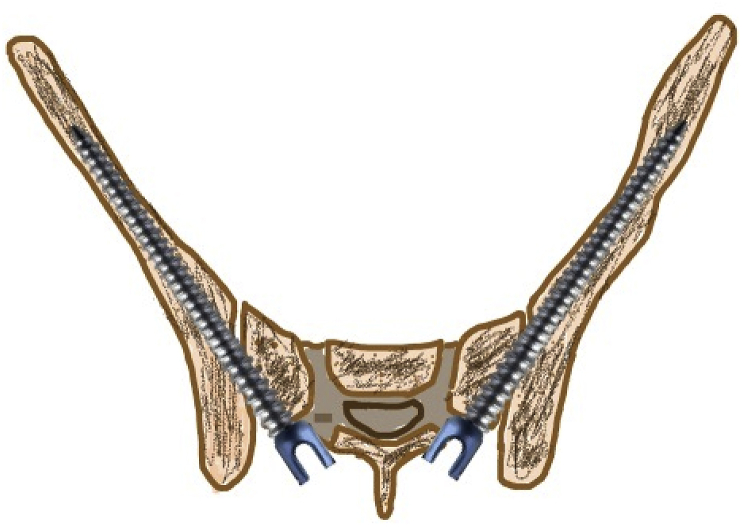
Sacropelvic is a complex junctional area owing to the complex regional anatomy and higher biomechanical stress. However extension of construct is indicated in cases with complex deformities, high grade spondylolisthesis, and complex fractures. The challenges remain which includes pseudoarthrosis and fixation failures. The fixation techniques have constantly evolved over time with better results with iliac screws and S2-alar-iliac screws. This article gives background on evolution, biomechanics, and recent update of use of robotics for sacropelvic fixation.
Keywords: Deformity; Fixation; Pelvic; Robotics; S2AI; Sacropelvic.
© 2020 Delhi Orthopedic Association. All rights reserved.
Figures


References
-
- Goodwin CR, Kosztowski TA, Elder BD, et al. Complex lumbosacropelvic fixation techniques. In: Steinmetz MP, Benzel EC, editors. Benzel’s Spine Surgery: Techniques, Complication Avoidance, and Management. Philadelphia, PA: Elsevier; 2017760e767.e2.
-
- Panjabi M.M., White A.A., III Basic biomechanics of the spine. Neurosurgery. 1980;7:76e93. - PubMed
-
- Dietrich M., Kurowski P. The importance of mechanical factors in the etiology of spondylolysis. A model analysis of loads and stresses in human lumbar spine. Spine (Phila Pa 1976) 1985;10:532e42. - PubMed
-
- Colombini D., Occhipinti E., Grieco A. Estimation of lumbar disc areas by means of anthropometric parameters. Spine (Phila Pa 1976) 1989;14:51e5. - PubMed
-
- Zheng Y., Lu W.W., Zhu Q. Variation in bone mineral density of the sacrum in young adults and its significance for sacral fixation. Spine (Phila Pa 1976) 2000;25:353e7. - PubMed
LinkOut - more resources
Full Text Sources
