

Clinical and pathological characteristics and prognosis of 132 cases of rectal neuroendocrine tumors
- PMID: 32879666
- PMCID: PMC7443838
- DOI: 10.4251/wjgo.v12.i8.893
Clinical and pathological characteristics and prognosis of 132 cases of rectal neuroendocrine tumors
Abstract
Background: Neuroendocrine tumors (NETs) frequently occur in the gastrointestinal tract, lung, and pancreas, and the rectum and appendix are the sites with the highest incidence. Epidemiology statistics show that an estimated 8000 people every year in the United States are diagnosed with NETs occurring in the gastrointestinal tract, including the stomach, intestine, appendix, colon, and rectum. The pathological changes and clinical symptoms of NETs are not specific, and therefore they are frequently misdiagnosed.
Aim: To investigate the clinical symptoms, pathological characteristics, treatment, and prognosis of rectal neuroendocrine tumors (RNETs) by analyzing the clinical and pathological data of 132 RNET cases at our hospital.
Methods: All RNETs were graded according to Ki-67 positivity and mitotic events. The tumors were staged as clinical stages I, II, III, and IV according to infiltrative depth and tumor size. COX proportional hazard model was used to assess the main risk factors for survival.
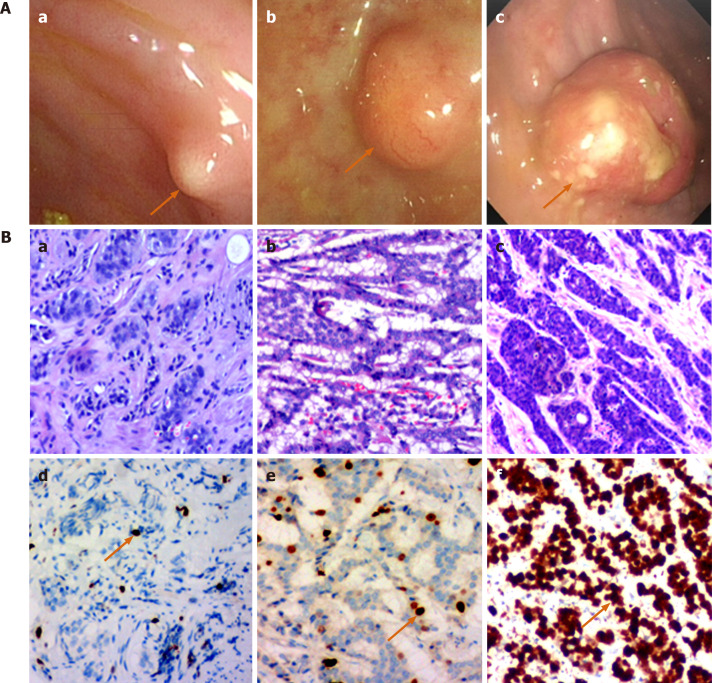
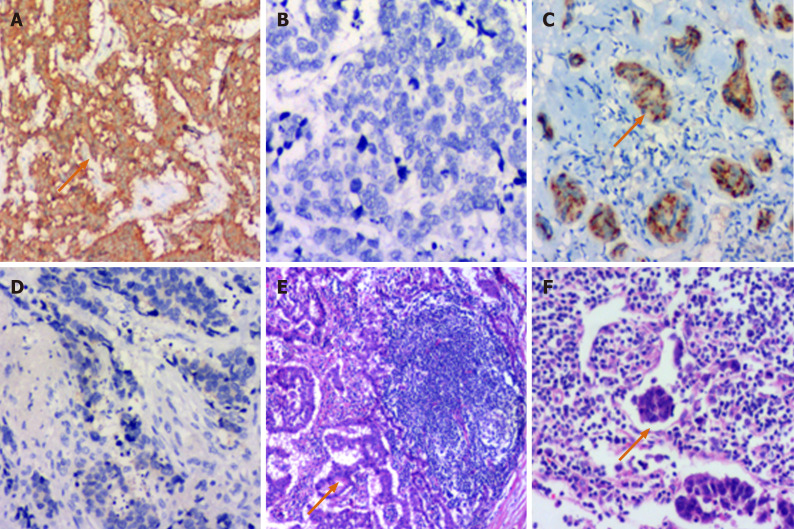
Results: These 132 RNETs included 83 cases of G1, 21 cases of G2, and 28 cases of G3 (neuroendocrine carcinoma) disease. Immunohistochemical staining showed that 89.4% of RNETs were positive for synaptophysin and 39.4% positive for chromogranin A. There were 19, 85, 23, and 5 cases of clinical stages I, II, III, and IV, respectively. The median patient age was 52.96 years. The diameter of tumor, depth of invasion, and pathological grade were the main reference factors for the treatment of RNETs. The survival rates at 6, 12, 36, and 60 mo after operation were 98.5%, 94.6%, 90.2%, and 85.6%, respectively. Gender, tumor size, tumor grade, lymph node or distant organ metastasis, and radical resection were the main factors associated with prognosis of RNETs. Multivariate analysis showed that tumor size and grade were independent prognostic factors.
Conclusion: The clinical symptoms of RNETs are not specific, and they are easy to misdiagnose. Surgery is the main treatment method. The grade and stage of RNETs are the main indices to evaluate prognosis.
Keywords: Neuroendocrine carcinoma; Neuroendocrine tumors; Prognosis; Tumor grade; Tumor size; Univariate analysis.
©The Author(s) 2020. Published by Baishideng Publishing Group Inc. All rights reserved.
Figures
Similar articles
-
Evaluation of the concordance between the stage of the disease and Ki-67 proliferation index in gastroenteropancreatic neuroendocrine tumors.Eur J Gastroenterol Hepatol. 2016 Jul;28(7):836-41. doi: 10.1097/MEG.0000000000000619. Eur J Gastroenterol Hepatol. 2016. PMID: 26945127
-
Risk factors for lymph node metastasis in rectal neuroendocrine tumors: A recursive partitioning analysis based on multicenter data.J Surg Oncol. 2021 Dec;124(7):1098-1105. doi: 10.1002/jso.26615. Epub 2021 Jul 22. J Surg Oncol. 2021. PMID: 34291822
-
Essentiality of Imaging Diagnostic Criteria Specific to Rectal Neuroendocrine Tumors for Detecting Metastatic Lymph Nodes.Anticancer Res. 2019 Jan;39(1):505-510. doi: 10.21873/anticanres.13141. Anticancer Res. 2019. PMID: 30591502
-
Risk factors for lateral pelvic lymph node metastasis in patients with rectal neuroendocrine tumors: a systematic review and meta-analysis.Front Oncol. 2025 Jan 31;15:1500623. doi: 10.3389/fonc.2025.1500623. eCollection 2025. Front Oncol. 2025. PMID: 39959663 Free PMC article.
-
Neuroendocrine neoplasms of the appendix, colon and rectum.Pathologica. 2021 Feb;113(1):19-27. doi: 10.32074/1591-951X-230. Pathologica. 2021. PMID: 33686307 Free PMC article. Review.
Cited by
-
Optimising Outcomes and Surveillance Strategies of Rectal Neuroendocrine Neoplasms.Cancers (Basel). 2023 May 15;15(10):2766. doi: 10.3390/cancers15102766. Cancers (Basel). 2023. PMID: 37345103 Free PMC article. Review.
-
Predictive and prognostic nomogram models for liver metastasis in colorectal neuroendocrine neoplasms: a large population study.Front Endocrinol (Lausanne). 2025 Jan 7;15:1488733. doi: 10.3389/fendo.2024.1488733. eCollection 2024. Front Endocrinol (Lausanne). 2025. PMID: 39839478 Free PMC article.
-
Evaluation of quality of clinical management of neuroendocrine tumors.Cancer Innov. 2022 Dec 16;1(4):305-315. doi: 10.1002/cai2.41. eCollection 2022 Dec. Cancer Innov. 2022. PMID: 38089084 Free PMC article.
-
Risk factors for lymph node metastasis and prognosis in colorectal neuroendocrine tumours.Int J Colorectal Dis. 2022 Feb;37(2):421-428. doi: 10.1007/s00384-021-04082-7. Epub 2022 Jan 8. Int J Colorectal Dis. 2022. PMID: 34997303 Free PMC article.
-
Prognostic Value of the Largest Lesion Size for Progression-Free Survival in Patients with NET Undergoing Salvage PRRT with [177Lu]Lu-DOTATOC.Cancers (Basel). 2022 Mar 31;14(7):1768. doi: 10.3390/cancers14071768. Cancers (Basel). 2022. PMID: 35406540 Free PMC article.
References
-
- Maschmeyer G, Mügge LO, Kämpfe D, Kreibich U, Wilhelm S, Aßmann M, Schwarz M, Kahl C, Köhler S, Grobe N, Niederwieser D. A retrospective review of diagnosis and treatment modalities of neuroendocrine tumors (excluding primary lung cancer) in 10 oncological institutions of the East German Study Group of Hematology and Oncology (OSHO), 2010-2012. J Cancer Res Clin Oncol. 2015;141:1639–1644. - PMC - PubMed
-
- Li ZS, Li Q. [The latest 2010 WHO classification of tumors of digestive system] Zhonghua Bing Li Xue Za Zhi. 2011;40:351–354. - PubMed
-
- Modlin IM, Lye KD, Kidd M. A 5-decade analysis of 13,715 carcinoid tumors. Cancer. 2003;97:934–959. - PubMed
-
- Landry CS, Brock G, Scoggins CR, McMasters KM, Martin RC 2nd. A proposed staging system for rectal carcinoid tumors based on an analysis of 4701 patients. Surgery. 2008;144:460–466. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
