

Association Between Body Size Phenotypes and Subclinical Atherosclerosis
- PMID: 32879953
- PMCID: PMC7521861
- DOI: 10.1210/clinem/dgaa620
Association Between Body Size Phenotypes and Subclinical Atherosclerosis
Abstract
Context: The underlying relationship between body mass index (BMI), cardiometabolic disorders, and subclinical atherosclerosis is poorly understood.
Objective: To evaluate the association between body size phenotypes and subclinical atherosclerosis.
Design: Cross-sectional.
Setting: Cardiovascular disease-free cohort.
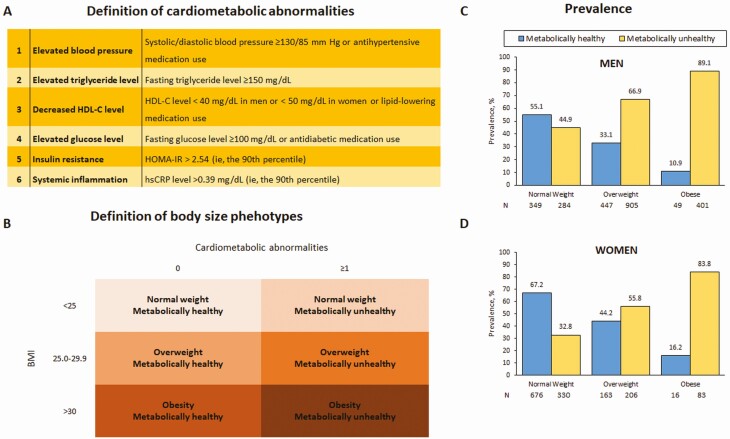
Participants: Middle-aged asymptomatic subjects (n = 3909). A total of 6 cardiometabolic body size phenotypes were defined based on the presence of at least 1 cardiometabolic abnormality (blood pressure, fasting blood glucose, triglycerides, low high-density lipoprotein cholesterol, homeostasis model assessment-insulin resistance index, high-sensitivity C-reactive protein) and based on BMI: normal-weight (NW; BMI <25), overweight (OW; BMI = 25.0-29.9) or obese (OB; BMI >30.0).
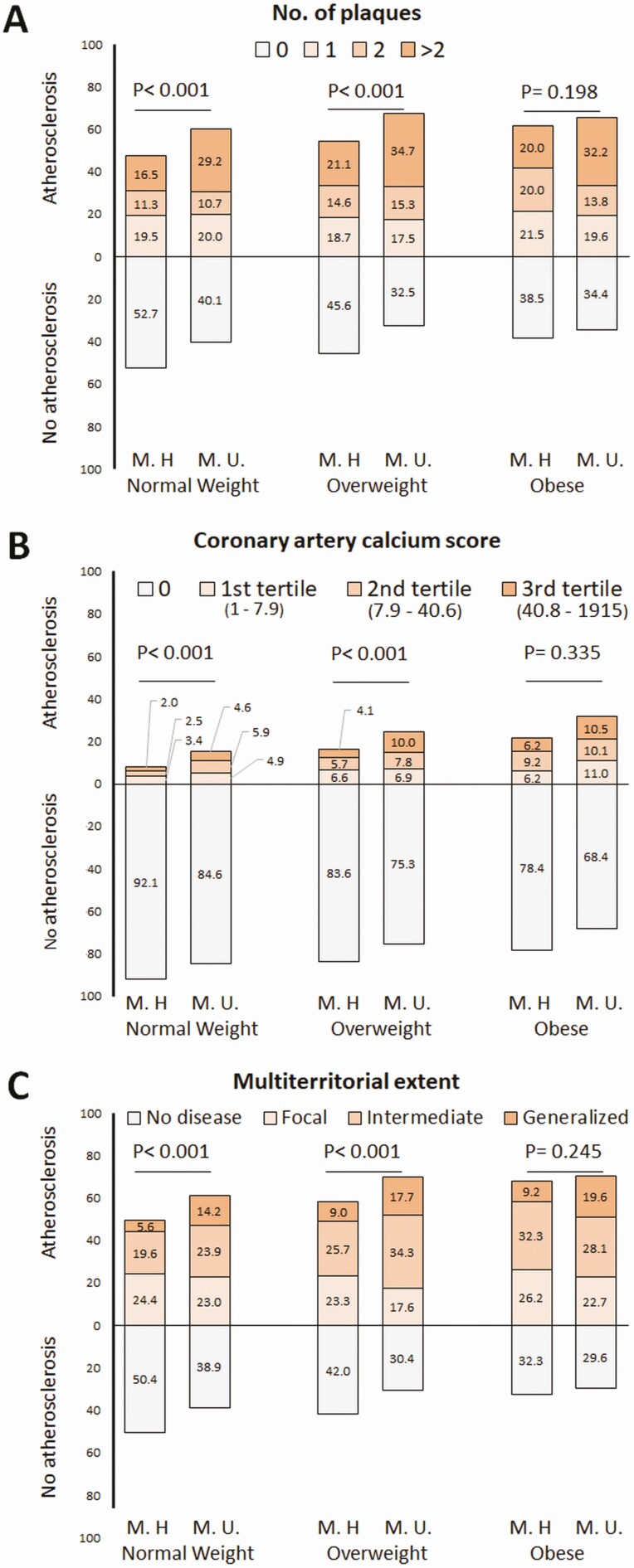
Main outcome measures: Subclinical atherosclerosis was evaluated by 2D vascular ultrasonography and noncontrast cardiac computed tomography.
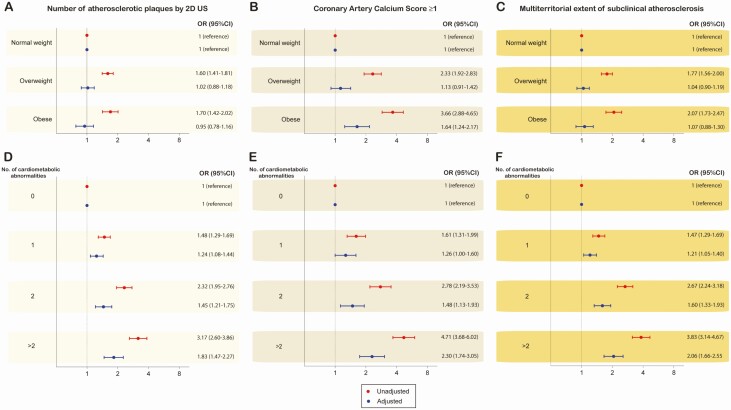
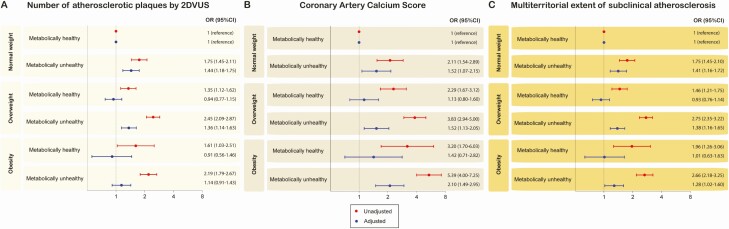
Results: For metabolically healthy subjects, the presence of subclinical atherosclerosis increased across BMI categories (49.6%, 58.0%, and 67.7% for NW, OW, and OB, respectively), whereas fewer differences were observed for metabolically unhealthy subjects (61.1%, 69.7%, and 70.5%, respectively). When BMI and cardiometabolic abnormalities were assessed separately, the association of body size phenotypes with the extent of subclinical atherosclerosis was mostly driven by the coexistence of cardiometabolic risk factors: adjusted OR = 1.04 (95% confidence interval [CI], 0.90-1.19) for OW and OR = 1.07 (95% CI, 0.88-1.30) for OB in comparison with NW, whereas there was an increasing association between the extent of subclinical atherosclerosis and the number of cardiometabolic abnormalities: adjusted OR = 1.21 (95% CI, 1.05-1.40), 1.60 (95% CI, 1.33-1.93), 1.92 (95% CI, 1.48-2.50), and 2.27 (95% CI, 1.67-3.09) for 1, 2, 3, and >3, respectively, in comparison with noncardiometabolic abnormalities.
Conclusions: The prevalence of subclinical atherosclerosis varies across body size phenotypes. Pharmacologic and lifestyle interventions might modify their cardiovascular risk by facilitating the transition from one phenotype to another.
Keywords: body size phenotypes; cardiovascular risk; obesity; subclinical atherosclerosis.
© Endocrine Society 2020.
Figures
References
-
- Blüher M. The distinction of metabolically ‘healthy’ from ‘unhealthy’ obese individuals. Curr Opin Lipidol. 2010;21(1):38-43. - PubMed
-
- Olshansky SJ, Passaro DJ, Hershow RC, et al. A potential decline in life expectancy in the United States in the 21st century. N Engl J Med. 2005;352(11):1138-1145. - PubMed
-
- Wildman RP, Muntner P, Reynolds K, et al. The obese without cardiometabolic risk factor clustering and the normal weight with cardiometabolic risk factor clustering: prevalence and correlates of 2 phenotypes among the US population (NHANES 1999-2004). Arch Intern Med. 2008;168(15):1617-1624. - PubMed
-
- Kramer CK, Zinman B, Retnakaran R. Are metabolically healthy overweight and obesity benign conditions?: A systematic review and meta-analysis. Ann Intern Med. 2013;159(11):758-769. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
