

Editorial
doi: 10.1007/s11239-020-02266-6.
Anticipating the long-term cardiovascular effects of COVID-19
Affiliations
- PMID: 32880795
- PMCID: PMC7467860
- DOI: 10.1007/s11239-020-02266-6
Item in Clipboard
Editorial
Anticipating the long-term cardiovascular effects of COVID-19
J Thromb Thrombolysis.
2020 Oct.
No abstract available
Figures
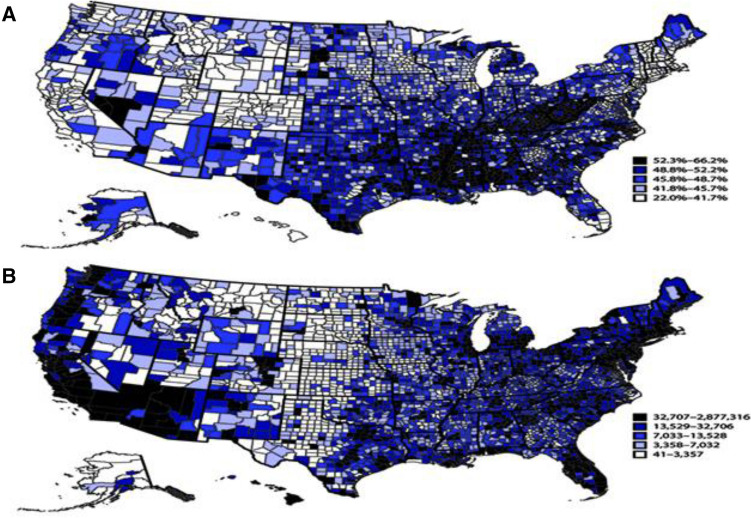
Map showing model-based estimates of United States prevalence a and number b of adults aged ≥ 18 years with any selected underlying medical condition, by county, in the United States, in 2018. *Selected underlying conditions include chronic obstructive pulmonary disease, emphysema, or chronic bronchitis; heart disease (angina or coronary heart disease, heart attack, or myocardial infarction); diabetes; chronic kidney disease; or obesity (body mass index ≥ 30 kg/m2). Adopted with permission from Ebinger [54]
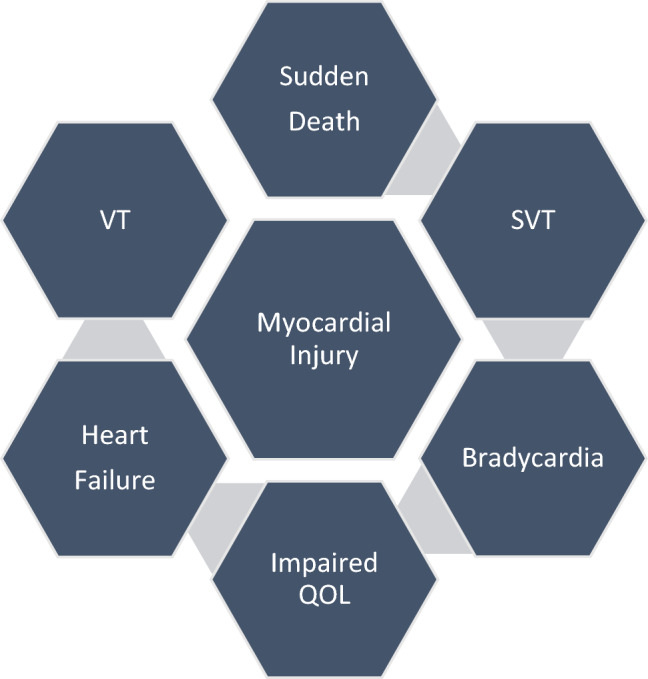
COVID-19 is associated with ischemic and non-ischemic myocardial injury that can be clinical or subclinical in the acute, subacute and chronic phases of SARS-CoV-2 infection. The risk for clinical events following initial recovery is under investigation, but monitoring and follow-up assessment should be integrated into the continuum of care to minimize the likelihood of life-threatening and life-altering events. VT ventricular tachycardia, SVT supraventricular tachycardia, QOL quality of life
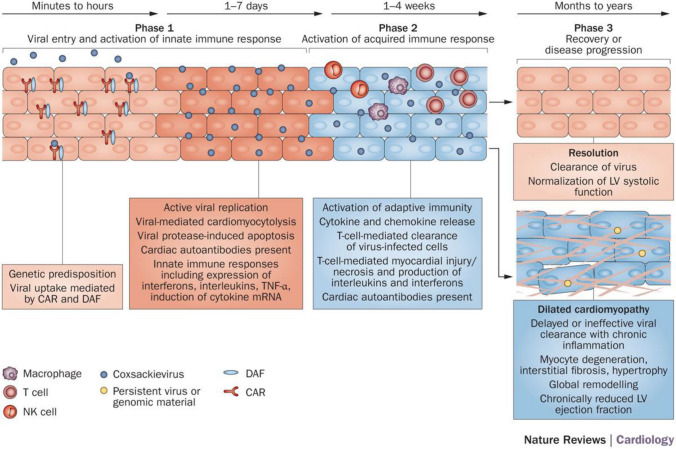
Phases of viral-associated cardiomyopathy: phase 1 commences with viral entry into the host and transit to the myocardium. In predisposed individuals, coxsackievirus binds to DAF on the cell surface, which shuttles the virus towards the CAR, localized at cell–cell junctions. The complex is internalized by the cell, triggering numerous cellular responses and activation of host innate immunity. Virus replication within the cardiomyocyte causes cell lysis, which prompts a set of cascades leading to the release of cytokines. In phase 2, both cellular and humoral responses contribute to autoimmune-mediated injury. The first immune cells recruited to the injured myocardium are NK cells, followed by macrophages. Infiltration of T cells typically peaks at 7–14 days; this timing coincides with the most severe phase of disease. As viral titer decrease, inflammation subsides (phase 3) and some individuals experience complete resolution of myocardial injury. However, in other patients, viral genomic material persists (in some cases up to 12 months; viral persistence throughout the entirety of end-stage disease until time of transplantation has been demonstrated), contributing to chronic inflammation and dilated cardiomyopathy. Abbreviations CAR coxsackievirus and adenovirus receptor, DAF decay accelerating factor, LV left ventricular, NK natural killer, TNF tumour necrosis factor. Adopted with permission from Pollack [14]
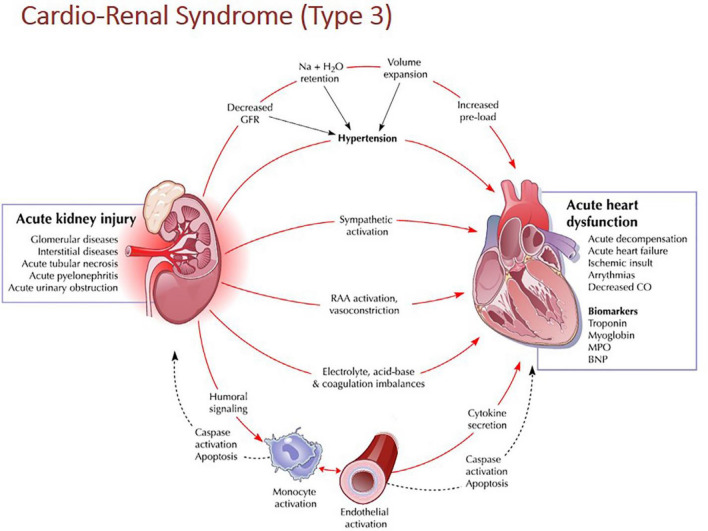
Pathophysiologic pathways in Type 3 cardiorenal syndrome. Acute Kidney Injury (AKI) is the initial insult in Type 3 CRS and can result from many potential etiologies. AKI is thought to have both direct and indirect effects on cardiac structure and function leading to acute cardiac injury. Direct mechanisms include RAA and SNS activation. Indirect mechanisms include volume overload, electrolyte disturbances, and acidemia. Acute cardiac injury can take multiple forms including acute heart failure, cardiac ischemia, and arrhythmia. Abbreviations BNP brain natriuretic peptide, GFR glomerular filtration rate, MPO myeloperoxidase, RAA renin–angiotensin–aldosterone, CRS cardiorenal syndrome. Adopted with permission from Ronco [30]
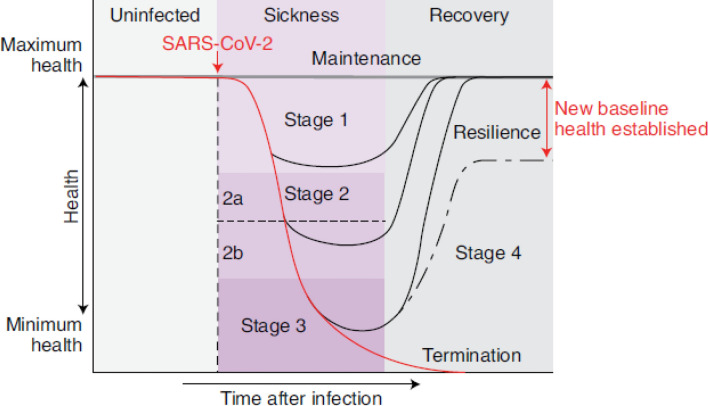
The disease phases of patients with COVID-19. After infection, patients can remain healthy and show no signs of sickness (maintenance of health). For patients who develop symptoms, the disease course can be described by four stages. Stage 1 is mild, and patients exhibit fever, malaise and a dry cough. Stage 2 is characterized by a pneumonia phase without or with hypoxia (2a, b). Patients who progress further along the disease course develop acute respiratory distress syndrome, shock or multiorgan failure (stage 3 III). Patients who recover (stage 4) from the infection show a resilience phenotype. Some patients may never return to their original health state, thus establishing a new baseline for health. Patients who peak in stages 1 or 2 will bypass stage 2 or 3, respectively, and enter into their recovery phase. Adopted with permission from Ayres [43]
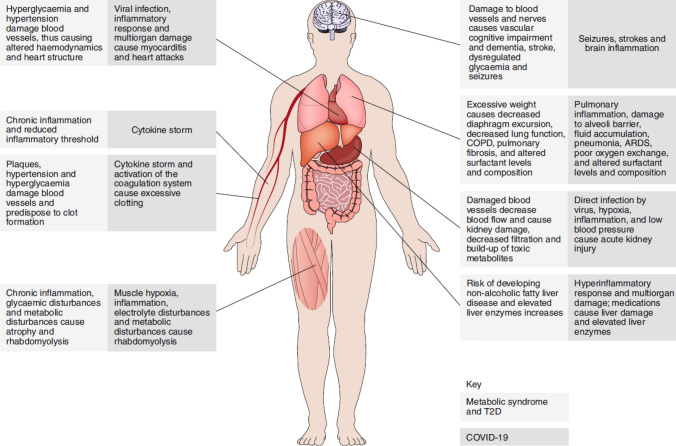
The parallels among metabolic syndrome, T2D and COVID-19. COVID-19, metabolic syndrome and T2D are multisystem diseases. The pathologies of metabolic syndrome and T2D affect the same systems that are damaged by COVID-19, thus predisposing patients to developing more severe pathology during the infection. We traditionally think about how metabolic syndrome and T2D make individuals more susceptible to infections because of diminished immune function, an understanding of the parallels between these conditions from a physiological perspective suggests that the greater susceptibility of these individuals to COVID-19 likely stems from an increased susceptibility to pathology and the resulting pathophysiology, rather than an inability to control the viral infection. COPD, chronic obstructive pulmonary disease, Type 2 diabetes mellitus (T2D). Adopted with permission from Ayres [43]
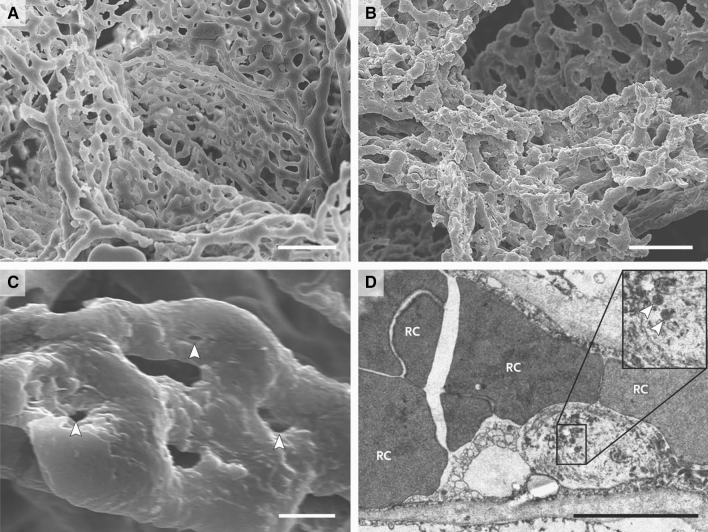
a, b Scanning electron micrographs of microvascular corrosion casts from the thin-walled alveolar plexus of a healthy lung (a) and the substantial architectural distortion seen in lungs injured by Covid-19 (b). The loss of a clearly visible vessel hierarchy in the alveolar plexus is the result of new blood-vessel formation by intussusceptive angiogenesis. c Shows the intussusceptive pillar localizations (arrowheads) at higher magnification. d Is a transmission electron micrograph showing ultrastructural features of endothelial cell destruction and SARS-CoV-2 visible within the cell membrane (arrowheads) (the scale bar corresponds to 5 μm). RC denotes red cell. Adopted with permission from Ackermann [52]
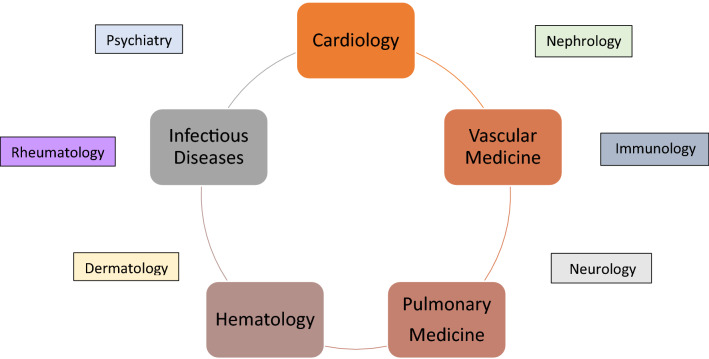
COVID-19 clinics for the diagnosis and management of patients with post-COVID-19 syndrome. The approach to patients with COVID-19 either following hospital discharge or a period of illness not requiring hospitalization but with symptoms is best configured and operationalized in a multi-disciplinary, dedicated clinic with broad expertise, established processes, standard operating procedures, resources and identity in the medical, referral and lay communities
References
-
- Wichmann D, Sperhake JP, Lütgehetmann M, Steurer S, Edler C, Heinemann A, Heinrich F, Mushumba H, Kniep I, Schröder AS, Burdelski C, de Heer G, Nierhaus A, Frings D, Pfefferle S, Becker H, Bredereke-Wiedling H, de Weerth A, Paschen HR, Sheikhzadeh-Eggers S, Stang A, Schmiedel S, Bokemeyer C, Addo MM, Aepfelbacher M, Püschel K, Kluge S. Autopsy findings and venous thromboembolism in patients with COVID-19: a prospective cohort study. Ann Intern Med. 2020;173:268–277. doi: 10.7326/M20-2003. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
