

Elevated Depressive Symptoms and the Risk of Stroke among the Mexican Older Population
- PMID: 32880905
- PMCID: PMC7745730
- DOI: 10.1111/jgs.16718
Elevated Depressive Symptoms and the Risk of Stroke among the Mexican Older Population
Abstract
Background/objectives: Several longitudinal studies in high-income countries suggest that depression increases stroke risk. However, few prior studies have evaluated this association in low- and middle-income countries (LMICs), where rapidly aging populations may have markedly different vascular risk profiles.
Design: Prospective cohort study.
Setting: The Mexican Health and Aging Study is a national population-based study of older adults in Mexico.
Participants: A total of 10,693 Mexican adults aged 50 and older enrolled in 2001 with no history of prior stroke.
Measurements: Depressive symptoms were assessed with a modified 9-item Centers for Epidemiologic Studies Depression Scale (elevated depressive symptom cutoff ≥5) in 2001 and 2003. We evaluated associations between baseline and short-term (2-year) changes in elevated depressive symptoms (categorized as stable low, recently remitted, recent-onset, or stable high symptoms) with incident self-reported or next-of-kin reported doctor-diagnosed stroke through 2015 using Cox proportional hazards models and sensitivity analyses applying inverse probability weights.
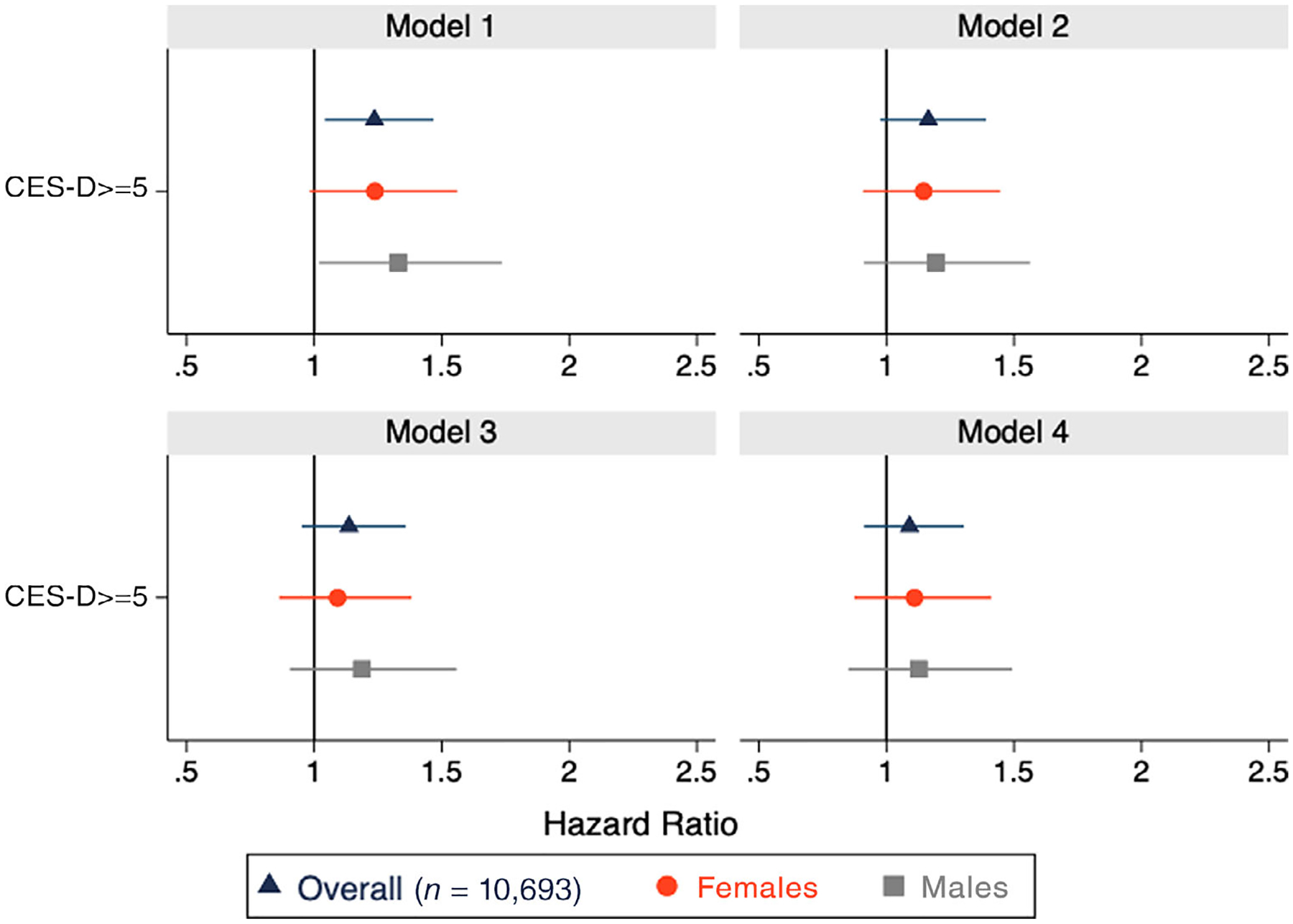
Results: Over an average follow-up of 11.4 years (standard deviation = 4.2), 10,693 respondents reported 546 incident strokes. Individuals with elevated baseline depressive symptoms experienced a moderately higher hazard of incident stroke (hazard ratio [HR] = 1.13; 95% confidence interval [CI] = .95-1.36) compared with those without elevated baseline depressive symptoms. In analyses of short-term changes in elevated depressive symptoms (n = 8,808; 414 incident stokes), participants with recent-onset (HR = 1.38; 95% CI = 1.06-1.81) or stable high (HR = 1.42; 95% CI = 1.10-1.84) elevated depressive symptoms had a greater hazard of incident stroke compared to those with stable low/no depressive symptoms, whereas recently remitted (HR = 1.01; 95% CI = .74-1.37) symptoms was not associated with stroke hazard.
Conclusion: Strategies to reduce depressive symptoms merit evaluation as approaches to prevent stroke in middle-income countries. Findings are similar to those in high-income countries but should be replicated in other LMICs.
Keywords: aging; depression; epidemiology; stroke.
© 2020 The American Geriatrics Society.
Conflict of interest statement
Figures

Similar articles
-
Prospective association between depressive symptoms and stroke risk among middle-aged and older Chinese.BMC Psychiatry. 2021 Oct 27;21(1):532. doi: 10.1186/s12888-021-03492-9. BMC Psychiatry. 2021. PMID: 34706692 Free PMC article.
-
Changes in Depressive Symptoms and Incidence of First Stroke Among Middle-Aged and Older US Adults.J Am Heart Assoc. 2015 May 13;4(5):e001923. doi: 10.1161/JAHA.115.001923. J Am Heart Assoc. 2015. PMID: 25971438 Free PMC article.
-
Changes in Depressive Symptoms and Subsequent Risk of Stroke in the Cardiovascular Health Study.Stroke. 2017 Jan;48(1):43-48. doi: 10.1161/STROKEAHA.116.013554. Epub 2016 Dec 6. Stroke. 2017. PMID: 27924053 Free PMC article.
-
Association of Depressive Symptoms With Incident Cardiovascular Diseases in Middle-Aged and Older Chinese Adults.JAMA Netw Open. 2019 Dec 2;2(12):e1916591. doi: 10.1001/jamanetworkopen.2019.16591. JAMA Netw Open. 2019. PMID: 31800066 Free PMC article.
-
Comparing Variability, Severity, and Persistence of Depressive Symptoms as Predictors of Future Stroke Risk.Am J Geriatr Psychiatry. 2017 Feb;25(2):120-128. doi: 10.1016/j.jagp.2016.10.009. Epub 2016 Oct 24. Am J Geriatr Psychiatry. 2017. PMID: 27866734 Free PMC article.
Cited by
-
Prevalence and incidence of stroke in Latin America and the Caribbean: a systematic review and meta-analysis.Sci Rep. 2023 Apr 26;13(1):6809. doi: 10.1038/s41598-023-33182-3. Sci Rep. 2023. PMID: 37100856 Free PMC article.
-
Prospective association between depressive symptoms and stroke risk among middle-aged and older Chinese.BMC Psychiatry. 2021 Oct 27;21(1):532. doi: 10.1186/s12888-021-03492-9. BMC Psychiatry. 2021. PMID: 34706692 Free PMC article.
-
Association between depression and stroke risk in adults: a systematic review and meta-analysis.Front Neurol. 2024 Apr 25;15:1331300. doi: 10.3389/fneur.2024.1331300. eCollection 2024. Front Neurol. 2024. PMID: 38725648 Free PMC article.
-
The longitudinal study of the relationship between social participation pattern and depression symptoms in frail older adults.Front Psychiatry. 2024 Sep 3;15:1440641. doi: 10.3389/fpsyt.2024.1440641. eCollection 2024. Front Psychiatry. 2024. PMID: 39290302 Free PMC article.
-
Incidence rate of stroke in Peru.Rev Peru Med Exp Salud Publica. 2021 Jul-Sep;38(3):399-405. doi: 10.17843/rpmesp.2021.383.7804. Epub 2021 Dec 20. Rev Peru Med Exp Salud Publica. 2021. PMID: 34932741 Free PMC article.
References
-
- Musselman DL, Evans DL, Nemeroff CB. The relationship of depression to cardiovascular disease: epidemiology, biology, and treatment. Arch Gen Psychiatry. 1998;55(7):580–592. - PubMed
-
- Shimbo D, Chaplin W, Crossman D, Haas D, Davidson KW. Role of depression and inflammation in incident coronary heart disease events. Am J Cardiol. 2005;96(7):1016–1021. - PubMed
-
- Howren MB, Lamkin DM, Suls J. Associations of depression with c-reactive protein, IL-1, and IL-6: a meta-analysis. Psychosom Med. 2009;71(2):171–186. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
