

Modulation of endothelial organelle size as an antithrombotic strategy
- PMID: 32881285
- PMCID: PMC8436738
- DOI: 10.1111/jth.15084
Modulation of endothelial organelle size as an antithrombotic strategy
Abstract
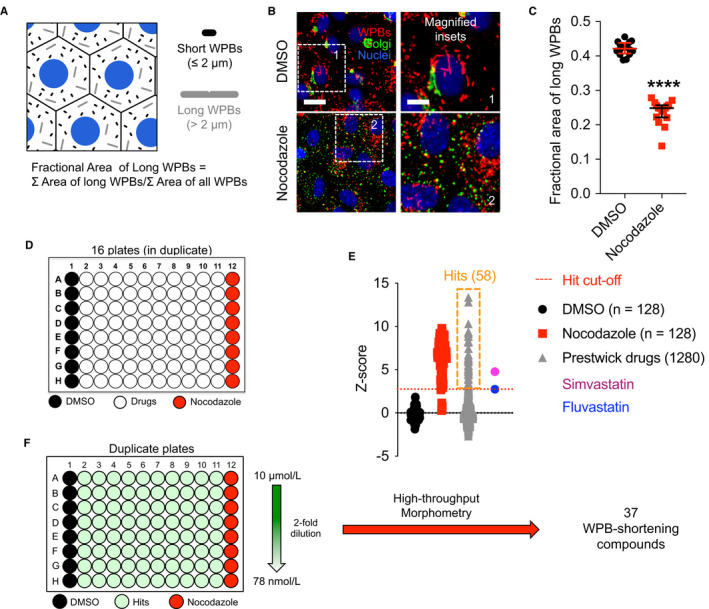
Background: It is long established that von Willebrand factor (VWF) is central to hemostasis and thrombosis. Endothelial VWF is stored in cell-specific secretory granules, Weibel-Palade bodies (WPBs), organelles generated in a wide range of lengths (0.5-5.0 µm). WPB size responds to physiological cues and pharmacological treatment, and VWF secretion from shortened WPBs dramatically reduces platelet and plasma VWF adhesion to an endothelial surface.
Objective: We hypothesized that WPB-shortening represented a novel target for antithrombotic therapy. Our objective was to determine whether compounds exhibiting this activity do exist.
Methods: Using a microscopy approach coupled to automated image analysis, we measured the size of WPB bodies in primary human endothelial cells treated with licensed compounds for 24 hours.
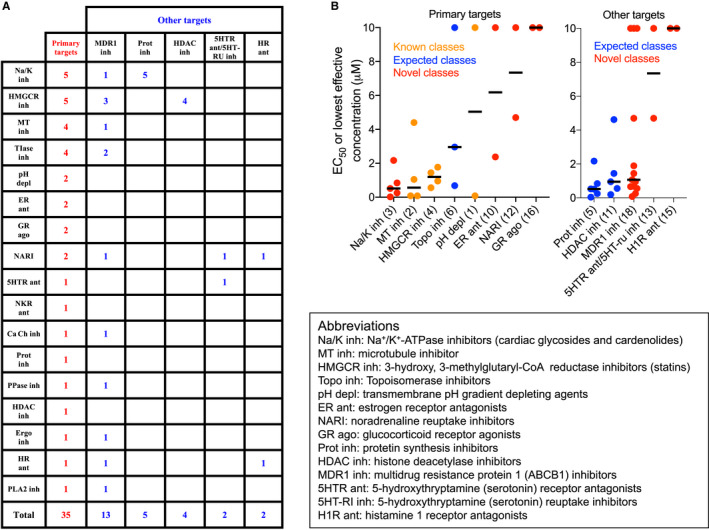
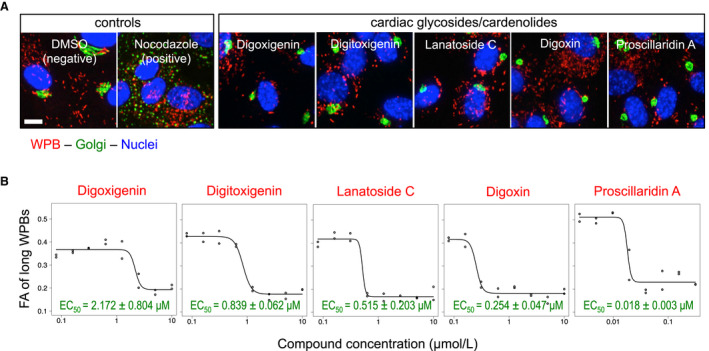
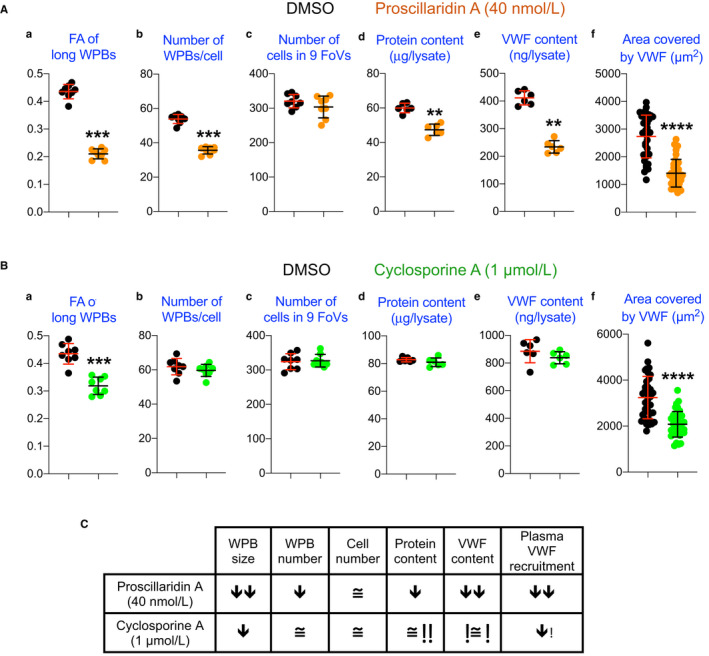
Results and conclusions: A novel approach to identification of antithrombotic compounds generated a significant number of candidates with the ability to shorten WPBs. In vitro assays of two selected compounds confirm that they inhibit the pro-hemostatic activity of secreted VWF. This set of compounds acting at a very early stage of the hemostatic process could well prove to be a useful adjunct to current antithrombotic therapeutics. Further, in the current SARS-CoV-2 pandemic, with a considerable fraction of critically ill COVID-19 patients affected by hypercoagulability, these WPB size-reducing drugs might also provide welcome therapeutic leads for frontline clinicians and researchers.
Keywords: COVID-19; Weibel-Palade bodies; drug repurposing; thrombosis; von Willebrand factor.
© 2020 The Authors. Journal of Thrombosis and Haemostasis published by Wiley Periodicals LLC on behalf of International Society on Thrombosis and Haemostasis.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
