

Postimplementation Evaluation of a Machine Learning-Based Deterioration Risk Alert to Enhance Sepsis Outcome Improvements
- PMID: 32881805
- PMCID: PMC10625790
- DOI: 10.1097/NAQ.0000000000000438
Postimplementation Evaluation of a Machine Learning-Based Deterioration Risk Alert to Enhance Sepsis Outcome Improvements
Abstract
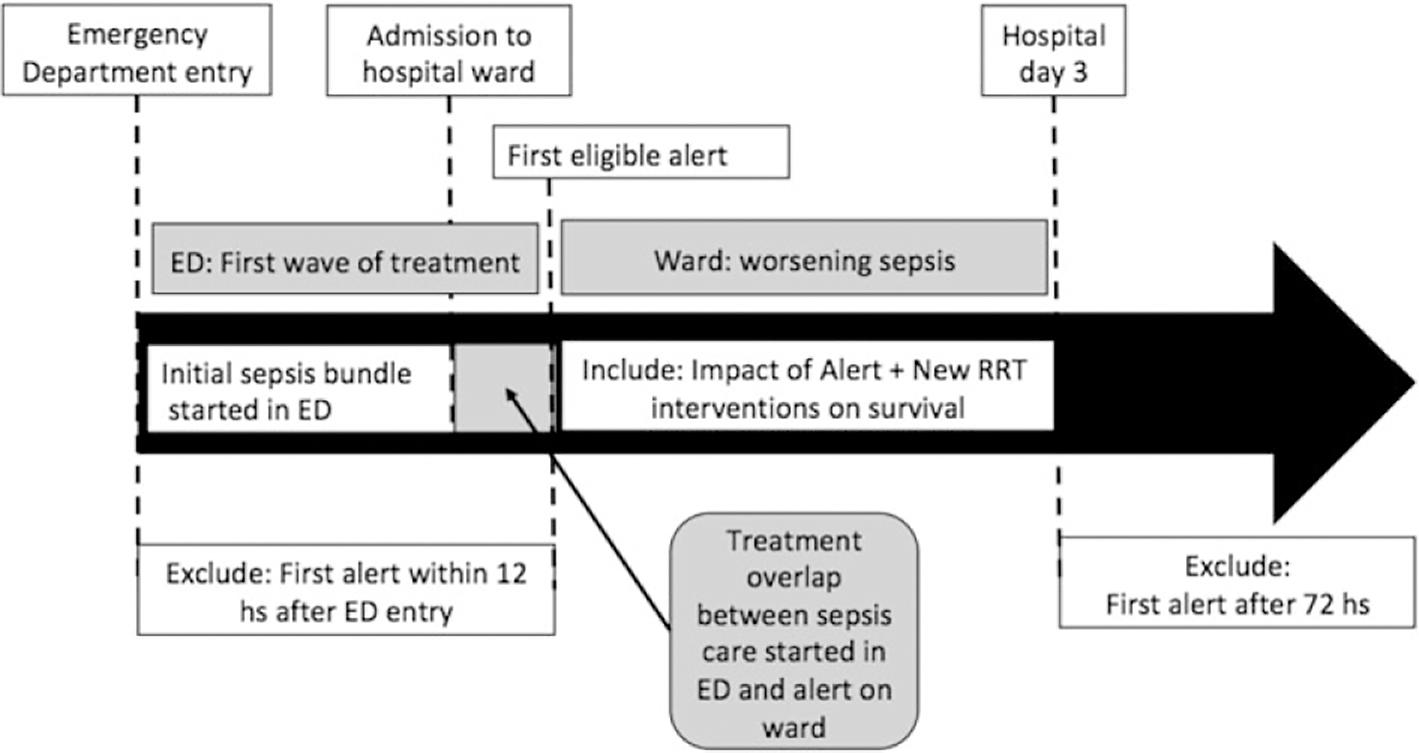
Machine learning-based early warning systems (EWSs) can detect clinical deterioration more accurately than point-score tools. In patients with sepsis, however, the timing and scope of sepsis interventions relative to an advanced EWS alert are not well understood. The objectives of this study were to evaluate the timing and frequency of fluid bolus therapy, new antibiotics, and Do Not Resuscitate (DNR) status relative to the time of an advanced EWS alert. We conducted 2 rounds of chart reviews of patients with an EWS alert admitted to community hospitals of a large integrated health system in Northern California (round 1: n = 21; round 2: n = 47). We abstracted patient characteristics and process measures of sepsis intervention and performed summary statistics. Sepsis decedents were older and sicker at admission and alert time. Most EWS alerts occurred near admission, and most sepsis interventions occurred before the first alert. Of 14 decedents, 12 (86%) had a DNR order before death. Fluid bolus therapy and new intravenous antibiotics frequently occurred before the alert, suggesting a potential overlap between sepsis care in the emergency department and the first alert following admission. Two tactics to minimize alerts that may not motivate new sepsis interventions are (1) locking out the alert during the immediate time after hospital admission; and (2) triaging and reviewing patients with alerts outside of the unit before activating a bedside response. Some decedents may have been on a palliative/end-of-life trajectory, because DNR orders were very common among decedents. Nurse leaders sponsoring or leading machine learning projects should consider tactics to reduce false-positive and clinically meaningless alerts dispatched to clinical staff.
Conflict of interest statement
Figures
Similar articles
-
Clinician Perception of a Machine Learning-Based Early Warning System Designed to Predict Severe Sepsis and Septic Shock.Crit Care Med. 2019 Nov;47(11):1477-1484. doi: 10.1097/CCM.0000000000003803. Crit Care Med. 2019. PMID: 31135500 Free PMC article.
-
Real-time machine learning-assisted sepsis alert enhances the timeliness of antibiotic administration and diagnostic accuracy in emergency department patients with sepsis: a cluster-randomized trial.Intern Emerg Med. 2024 Aug;19(5):1415-1424. doi: 10.1007/s11739-024-03535-5. Epub 2024 Feb 21. Intern Emerg Med. 2024. PMID: 38381351 Clinical Trial.
-
Clinical evaluation of a machine learning-based early warning system for patient deterioration.CMAJ. 2024 Sep 15;196(30):E1027-E1037. doi: 10.1503/cmaj.240132. CMAJ. 2024. PMID: 39284602 Free PMC article.
-
Sepsis Alerts in Emergency Departments: A Systematic Review of Accuracy and Quality Measure Impact.West J Emerg Med. 2020 Aug 24;21(5):1201-1210. doi: 10.5811/westjem.2020.5.46010. West J Emerg Med. 2020. PMID: 32970576 Free PMC article.
-
Statistical Modeling and Aggregate-Weighted Scoring Systems in Prediction of Mortality and ICU Transfer: A Systematic Review.J Hosp Med. 2019 Mar;14(3):161-169. doi: 10.12788/jhm.3151. J Hosp Med. 2019. PMID: 30811322 Free PMC article.
Cited by
-
Information displays for automated surveillance algorithms of in-hospital patient deterioration: a scoping review.J Am Med Inform Assoc. 2023 Dec 22;31(1):256-273. doi: 10.1093/jamia/ocad203. J Am Med Inform Assoc. 2023. PMID: 37847664 Free PMC article.
References
-
- Gaieski DF, Edwards JM, Kallan MJ, Carr BG. Benchmarking the incidence and mortality of severe sepsis in the United States. Crit Care Med. 2013;41(5):1167–1174. - PubMed
-
- Epstein L, Dantes R, Magill S, Fiore A. Varying Estimates of Sepsis Mortality Using Death Certificates and Administrative Codes—United States, 1999–2014. Atlanta, GA: Centers for Disease Control and Prevention; 2016. - PubMed
-
- Engel C, Brunkhorst FM, Bone HG, et al. Epidemiology of sepsis in Germany: results from a national prospective multicenter study. Intensive Care Med. 2007;33(4):606–618. - PubMed
-
- Liu V, Escobar G, Greene J, et al. Hospital deaths in patients with sepsis from 2 independent cohorts. JAMA. 2014;312(1):90–92. - PubMed
-
- Healthcare Cost Utilization Project. HCUP facts and figures. In: HCUP Facts and Figures, 2006: Statistics on Hospital-Based Care in the United States. Rockville, MD: Agency for Healthcare Research and Quality; 2008:38–41. https://www.hcup-us.ahrq.gov/reports/factsandfigures/HAR_2006.pdf. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
