

Lung ultrasound score in establishing the timing of intubation in COVID-19 interstitial pneumonia: A preliminary retrospective observational study
- PMID: 32881950
- PMCID: PMC7470341
- DOI: 10.1371/journal.pone.0238679
Lung ultrasound score in establishing the timing of intubation in COVID-19 interstitial pneumonia: A preliminary retrospective observational study
Retraction in
-
Retraction: Lung ultrasound score in establishing the timing of intubation in COVID-19 interstitial pneumonia: A preliminary retrospective observational study.PLoS One. 2020 Dec 31;15(12):e0245032. doi: 10.1371/journal.pone.0245032. eCollection 2020. PLoS One. 2020. PMID: 33382851 Free PMC article. No abstract available.
Expression of concern in
-
Expression of Concern: Lung ultrasound score in establishing the timing of intubation in COVID-19 interstitial pneumonia: A preliminary retrospective observational study.PLoS One. 2020 Nov 30;15(11):e0243267. doi: 10.1371/journal.pone.0243267. eCollection 2020. PLoS One. 2020. PMID: 33253279 Free PMC article. No abstract available.
Abstract
Purpose: To investigate the role of lung ultrasound score (LUS) in assessing intubation timing for patients with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pneumonia.
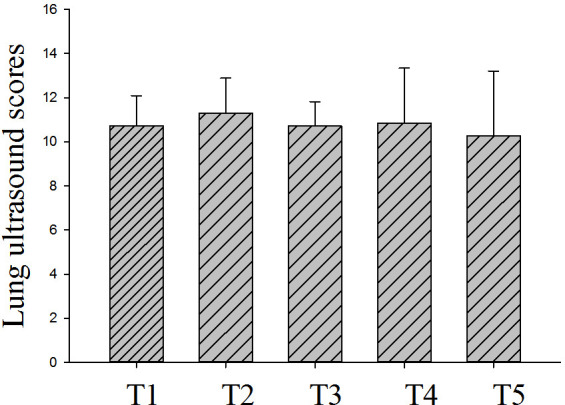
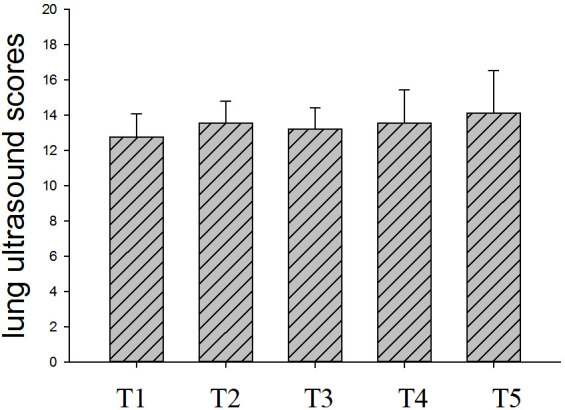
Materials and methods: Seventy-two patients with critical coronavirus disease 2019 (COVID-19) were admitted to a makeshift intensive care unit (ICU). All patients underwent bedside lung ultrasonography one to two times per day. The patients were either intubated, treated with noninvasive ventilation (NIV), or given high-flow nasal cannula (HFNC) after a discussion with the multidisciplinary group after their conditions worsened. Bedside lung ultrasound was performed daily after intubation, and patients received mechanical ventilation. Lung ultrasound was performed on days 1, 2, 3, 5, and 7 after patients were admitted to the ICU; if the patient was intubated, LUS determination was performed before intubation within 24 h (T1) and on days 1, 2, 5, and 7 after intubation (T2, T3, T4, and T5, respectively).The goal of this study was to evaluate the severity of lung aeration loss in intubated and non-intubated patients with SARS-CoV-2 pneumonia by ultrasound at different time points within one week.
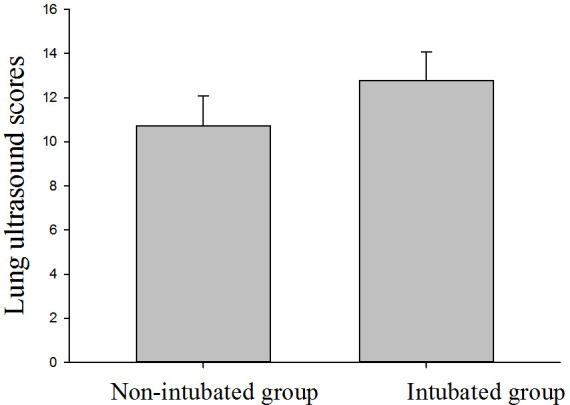
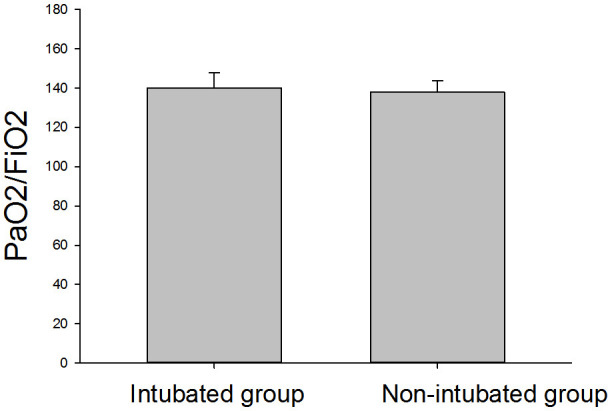
Results: A total of 16 patients were included in this study, including nine who were intubated and mechanically ventilated and seven patients without intubation. The number of elderly individuals in the intubated group was higher than in the non-intubated group (P < 0.05). In addition, there were more male than female patients in both groups. Patient characteristics (BMI, SOFA, and PaO2/FiO2 value) were similar between the two groups (P > 0.05). The 28-day mortality rate of intubated patients was higher than that of non-intubated patients; six patients in the intubated group and two patients in the non-intubated group died. Nine intubated patients showed changes in LUS within seven days (n = 9). The mean LUS within 24 h before intubation was 12.8 ± 1.3. LUS was significantly higher on T1 than on T5 (P <0.05), and did not significantly differ from T1 to T4. Comparing LUS between intubated and non-intubated patients on T1 showed that the LUS of intubated patients was significantly higher than that of non-intubated patients (P <0.05). Between the two patient groups, oxygenation index was 140.1 ± 7.7 vs. 137.8 ± 5.9 on T1, and the respiratory rate of the two groups was 26 ± 5 vs. 28 ± 4 breaths/min. Neither oxygenation index nor RR significantly differed between the two groups.
Conclusion: LUS may be an effective tool for assessing intubation timing in critically ill patients with Covid-19 interstitial pneumonia.
Conflict of interest statement
The author(s) received no specific funding for this work.
Figures
References
-
- Gorbalenya AE, Baker SC, Baric RS, et al. Severe acute respiratory syndrome-related coronavirus: the species and its viruses—a statement of the Coronavirus Study Group. bioRxiv 2020; published online Feb 11.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
