

Persisting Muscle Dysfunction in Cushing's Syndrome Despite Biochemical Remission
- PMID: 32882010
- PMCID: PMC7538105
- DOI: 10.1210/clinem/dgaa625
Persisting Muscle Dysfunction in Cushing's Syndrome Despite Biochemical Remission
Abstract
Context: Glucocorticoid-induced myopathy is a characteristic symptom of endogenous Cushing's syndrome (CS). Its long-term outcome is largely unknown.
Objective: To evaluate long-term muscle function following the remission of endogenous CS.
Study design: Observational longitudinal cohort study.
Setting: Tertiary care hospitals and a specialized outpatient clinic.
Patients: As part of the prospective multicenter German Cushing's Registry, we assessed muscle strength in patients with overt endogenous CS. We studied the patients at the time of diagnosis (n = 88), after 6 months (n = 69), and thereafter annually, following surgical remission over a period of up to 4 years (1 year: n = 55; 2 years: n = 34; 3 years: n = 29; 4 years: n = 22). Muscle function was evaluated by hand grip strength and by chair rising test.
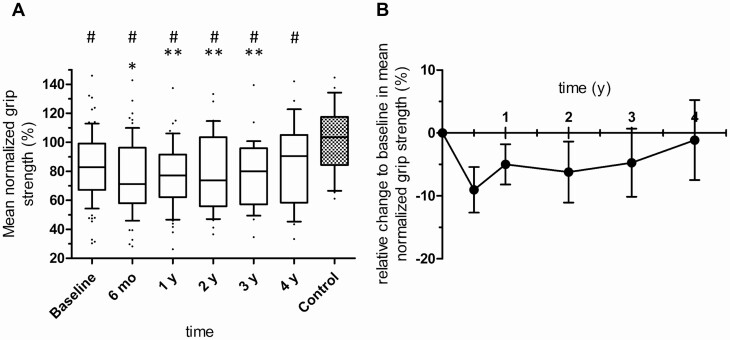
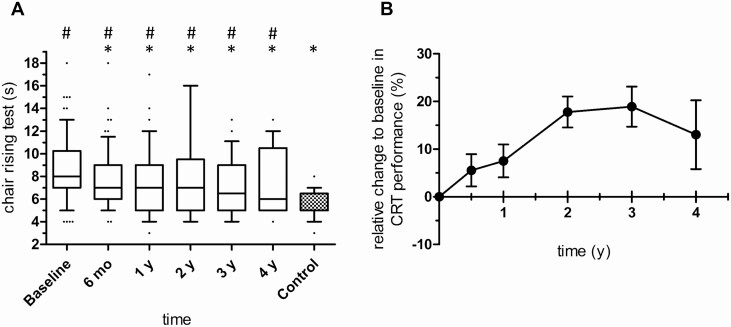
Results: Grip strength was decreased to 83% of normal controls (100%) at the time of diagnosis. It further decreased to 71% after 6 months in remission (P ≤ 0.001) and showed no improvement during further follow-up compared with baseline. Chair rising test performance improved initially (8 seconds at baseline vs 7 seconds after 6 months, P = 0.004) but remained at this reduced level thereafter (7 seconds after 3 years vs 5 seconds in controls, P = 0.038). In multivariate analysis, we identified, as predictors for long-term muscle dysfunction, age, waist-to-hip ratio, and hemoglobin A1c at baseline. Furthermore, muscle strength during follow-up was strongly correlated with quality of life.
Conclusion: This study shows that CS-associated myopathy does not spontaneously resolve during remission. This calls for action to identify effective interventions to improve muscle dysfunction in this setting.
Keywords: ACTH; cortisol; diabetes; hypercortisolism; muscle; sarcopenia.
© Endocrine Society 2020.
Figures
Similar articles
-
Persistence of myopathy in Cushing's syndrome: evaluation of the German Cushing's Registry.Eur J Endocrinol. 2017 Jun;176(6):737-746. doi: 10.1530/EJE-16-0689. Epub 2017 Mar 21. Eur J Endocrinol. 2017. PMID: 28325824
-
Patients with low IGF-I after curative surgery for Cushing's syndrome have an adverse long-term outcome of hypercortisolism-induced myopathy.Eur J Endocrinol. 2021 May 4;184(6):813-821. doi: 10.1530/EJE-20-1285. Eur J Endocrinol. 2021. PMID: 33830940
-
Glucocorticoid Receptor Polymorphisms Influence Muscle Strength in Cushing's Syndrome.J Clin Endocrinol Metab. 2020 Jan 1;105(1):dgz052. doi: 10.1210/clinem/dgz052. J Clin Endocrinol Metab. 2020. PMID: 31613324
-
Improvement in cognitive impairment following the successful treatment of endogenous Cushing's syndrome-a case report and literature review.BMC Endocr Disord. 2019 Jun 28;19(1):68. doi: 10.1186/s12902-019-0401-4. BMC Endocr Disord. 2019. PMID: 31253144 Free PMC article. Review.
-
Association of hypertension and hypokalemia with Cushing's syndrome caused by ectopic ACTH secretion: a series of 58 cases.Ann N Y Acad Sci. 2002 Sep;970:134-44. doi: 10.1111/j.1749-6632.2002.tb04419.x. Ann N Y Acad Sci. 2002. PMID: 12381548 Review.
Cited by
-
Metformin and Bone Metabolism in Endogenous Glucocorticoid Excess: An Exploratory Study.Front Endocrinol (Lausanne). 2021 Oct 27;12:765067. doi: 10.3389/fendo.2021.765067. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 34777259 Free PMC article.
-
Screening of hypercortisolism among patients with hypertension: an Italian nationwide survey.J Endocrinol Invest. 2024 Dec;47(12):3029-3038. doi: 10.1007/s40618-024-02387-2. Epub 2024 Jun 24. J Endocrinol Invest. 2024. PMID: 38913251 Free PMC article.
-
11-beta-hydroxysteroid dehydrogenase type 1 (HSD11B1) gene expression in muscle is linked to reduced skeletal muscle index in sarcopenic patients.Aging Clin Exp Res. 2023 Dec;35(12):3073-3083. doi: 10.1007/s40520-023-02574-w. Epub 2023 Nov 9. Aging Clin Exp Res. 2023. PMID: 37943405 Free PMC article.
-
Challenges in the postsurgical recovery of cushing syndrome: glucocorticoid withdrawal syndrome.Front Endocrinol (Lausanne). 2024 Apr 12;15:1353543. doi: 10.3389/fendo.2024.1353543. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38681763 Free PMC article. Review.
-
Consensus on diagnosis and management of Cushing's disease: a guideline update.Lancet Diabetes Endocrinol. 2021 Dec;9(12):847-875. doi: 10.1016/S2213-8587(21)00235-7. Epub 2021 Oct 20. Lancet Diabetes Endocrinol. 2021. PMID: 34687601 Free PMC article. Review.
References
-
- Pecori Giraldi F, Moro M, Cavagnini F; Study Group on the Hypothalamo-Pituitary-Adrenal Axis of the Italian Society of Endocrinology . Gender-related differences in the presentation and course of Cushing’s disease. J Clin Endocrinol Metab. 2003;88(4):1554–1558. - PubMed
-
- Pereira RM, Freire de Carvalho J. Glucocorticoid-induced myopathy. Joint Bone Spine. 2011;78(1):41–44. - PubMed
-
- Minetto MA, Lanfranco F, Motta G, Allasia S, Arvat E, D’Antona G. Steroid myopathy: some unresolved issues. J Endocrinol Invest. 2011;34(5):370–375. - PubMed
-
- Minetto MA, Caresio C, Salvi M, et al. Ultrasound-based detection of glucocorticoid-induced impairments of muscle mass and structure in Cushing’s disease. J Endocrinol Invest. 2019;42(7):757–768. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
