

Impaired angiotensin II type 1 receptor signaling contributes to sepsis-induced acute kidney injury
- PMID: 32882263
- PMCID: PMC8030124
- DOI: 10.1016/j.kint.2020.07.047
Impaired angiotensin II type 1 receptor signaling contributes to sepsis-induced acute kidney injury
Abstract
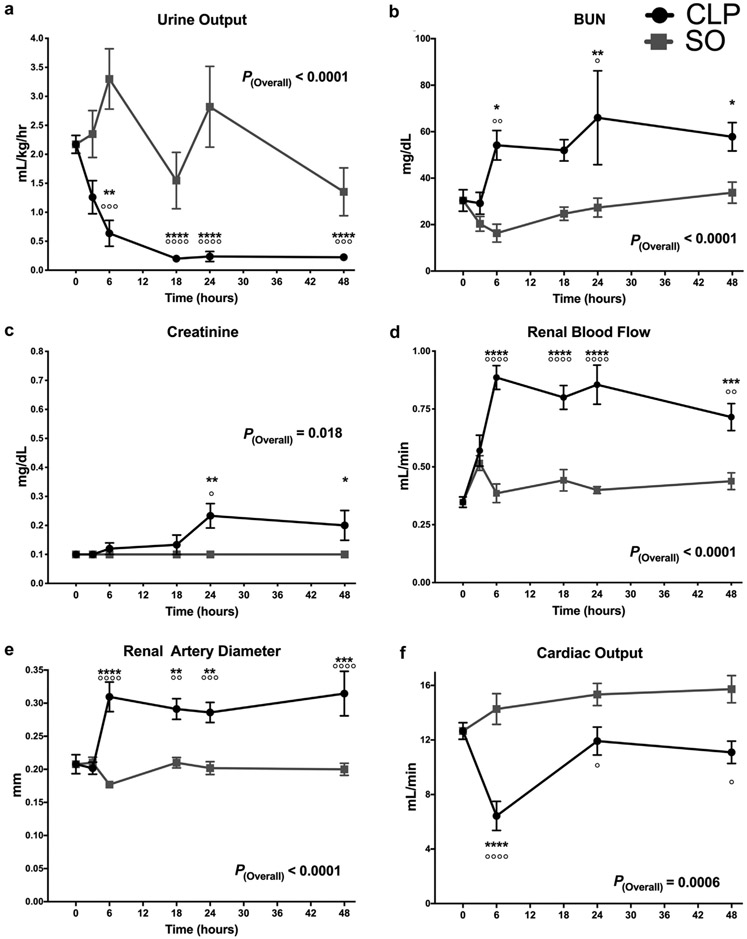
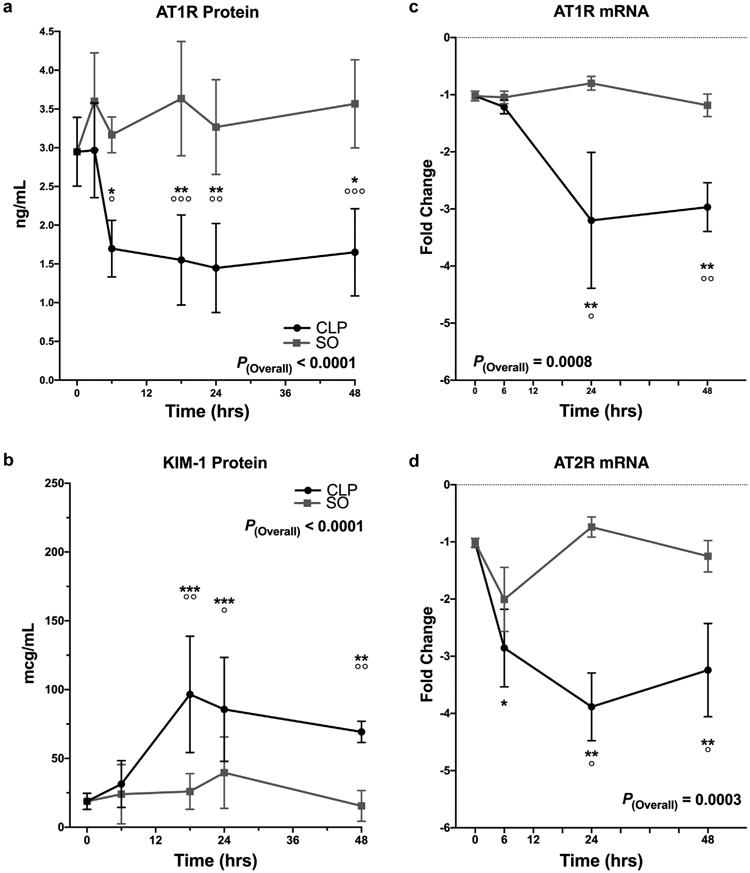
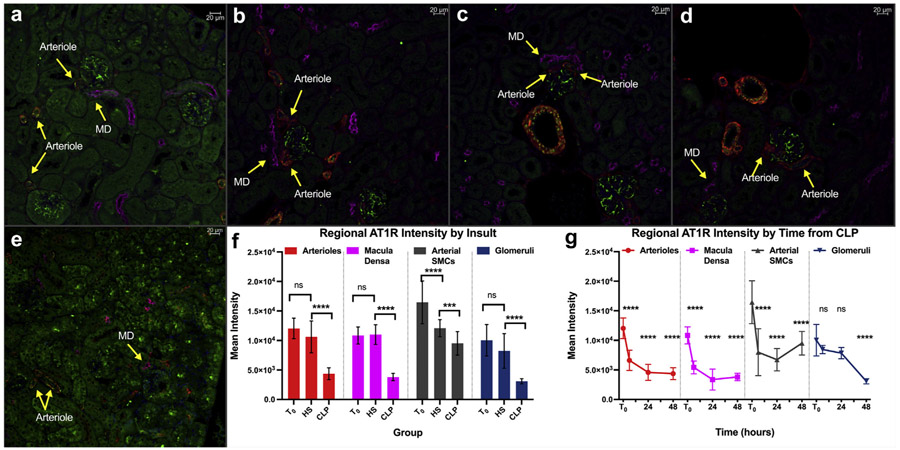
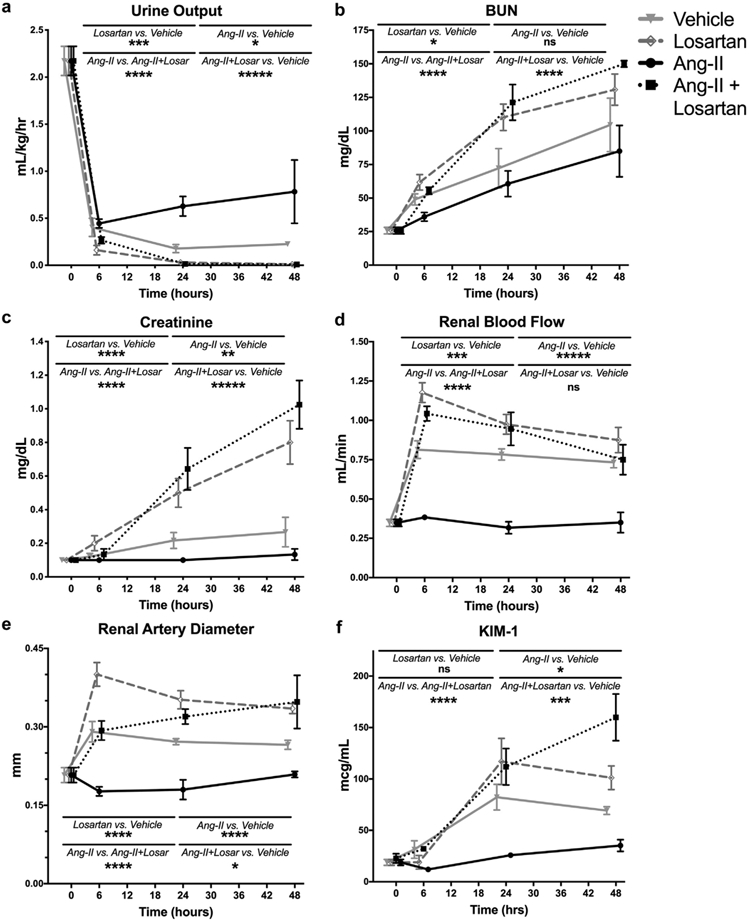
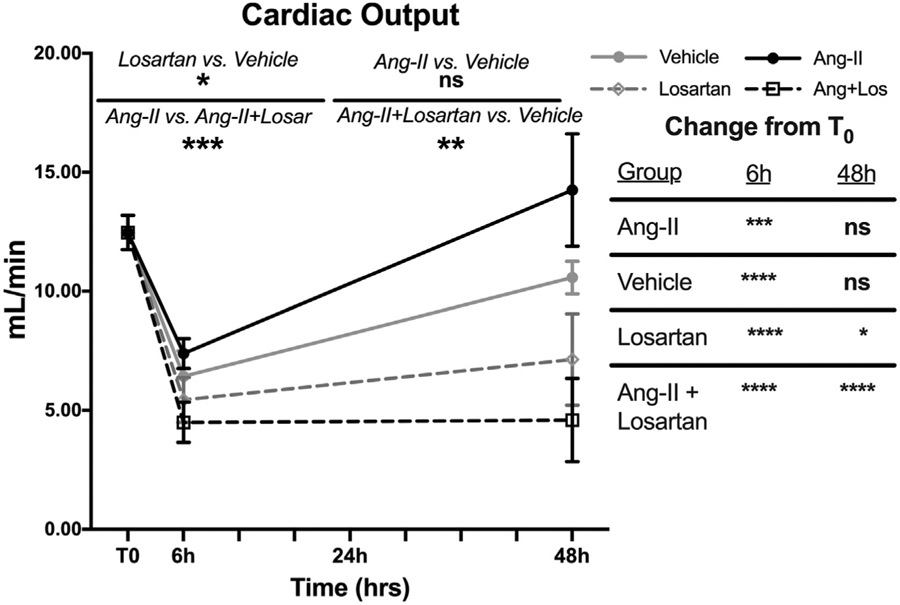
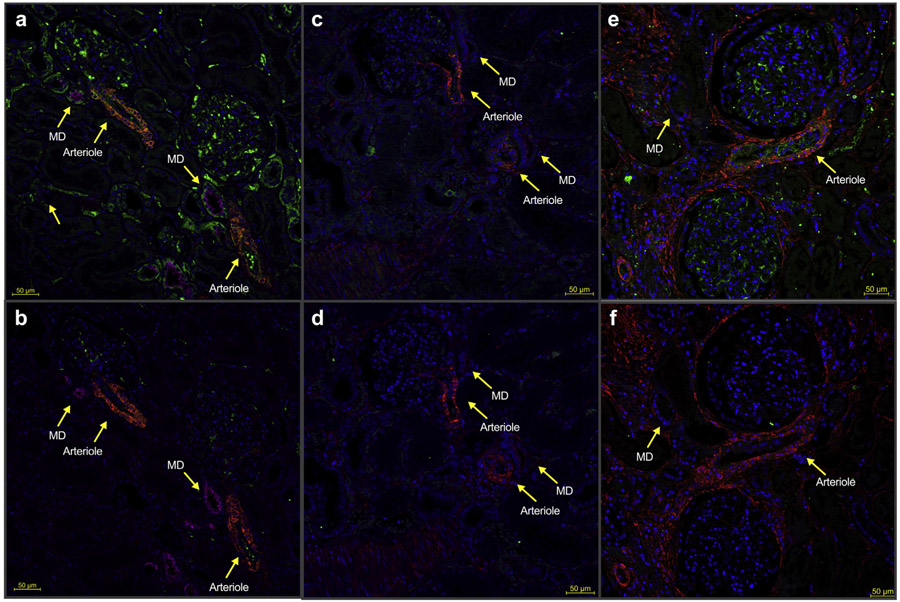
In sepsis-induced acute kidney injury, kidney blood flow may increase despite decreased glomerular filtration. Normally, angiotensin-II reduces kidney blood flow to maintain filtration. We hypothesized that sepsis reduces angiotensin type-1 receptor (AT1R) expression to account for this observation and tested this hypothesis in a patient case-control study and studies in mice. Seventy-three mice underwent cecal ligation and puncture (a sepsis model) or sham operation. Additionally, 94 septic mice received losartan (selective AT1R antagonist), angiotensin II without or with losartan, or vehicle. Cumulative urine output, kidney blood flow, blood urea nitrogen, and creatinine were measured. AT1R expression was assessed using ELISA, qPCR, and immunofluorescence. A blinded pathologist evaluated tissue for ischemic injury. AT1R expression was compared in autopsy tissue from seven patients with sepsis to that of the non-involved portion of kidney from ten individuals with kidney cancer and three non-infected but critically ill patients. By six hours post ligation/puncture, kidney blood flow doubled, blood urea nitrogen rose, and urine output fell. Concurrently, AT1R expression significantly fell 2-fold in arterioles and the macula densa. Creatinine significantly rose by 24 hours and sham operation did not alter measurements. Losartan significantly exacerbated ligation/puncture-induced changes in kidney blood flow, blood urea nitrogen, creatinine, and urine output. There was no histologic evidence of cortical ischemia. Significantly, angiotensin II prevented changes in kidney blood flow, creatinine, and urine output compared to vehicle. Co-administering losartan with angiotensin-II reversed this protection. Relative to both controls, patients with sepsis had low AT1R expression in arterioles and macula densa. Thus, murine cecal ligation/puncture and clinical sepsis decrease renal AT1R expression. Angiotensin II prevents functional changes while AT1R-blockade exacerbates them independent of ischemia in mice.
Keywords: acute kidney injury; angiotensin II; receptor, angiotensin, type 1; sepsis.
Copyright © 2020 International Society of Nephrology. Published by Elsevier Inc. All rights reserved.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
