

Potential Lipid Signatures for Diagnosis and Prognosis of Sepsis and Systemic Inflammatory Response Syndrome
- PMID: 32882869
- PMCID: PMC7570015
- DOI: 10.3390/metabo10090359
Potential Lipid Signatures for Diagnosis and Prognosis of Sepsis and Systemic Inflammatory Response Syndrome
Abstract
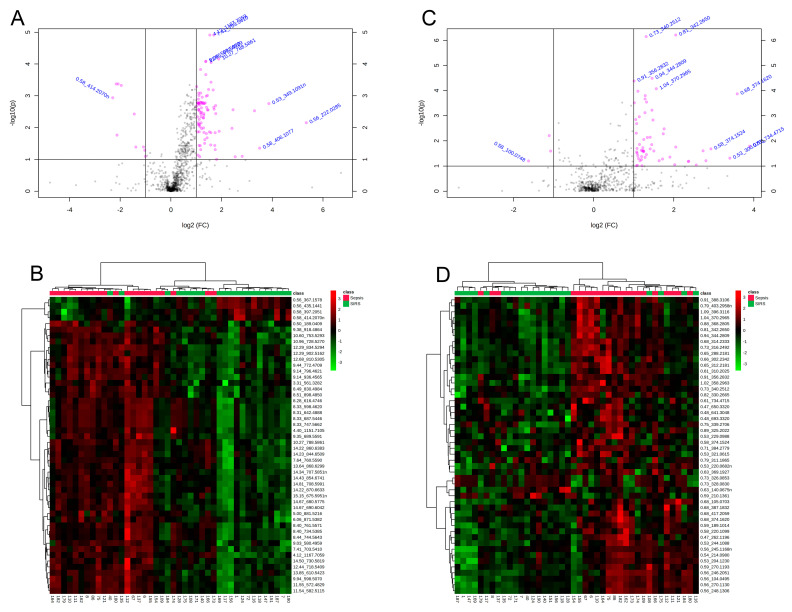
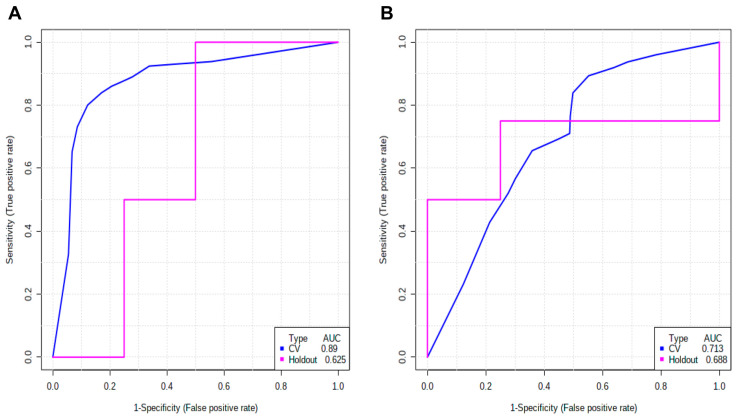
Systemic inflammatory response syndrome (SIRS) and sepsis are two conditions which are difficult to differentiate clinically and which are strongly impacted for prompt intervention. This study identified potential lipid signatures that are able to differentiate SIRS from sepsis and to predict prognosis. Forty-two patients, including 21 patients with sepsis and 21 patients with SIRS, were involved in the study. Liquid chromatography coupled to mass spectrometry and multivariate statistical methods were used to determine lipids present in patient plasma. The obtained lipid signatures revealed 355 features for the negative ion mode and 297 for the positive ion mode, which were relevant for differential diagnosis of sepsis and SIRS. These lipids were also tested as prognosis predictors. Lastly, L-octanoylcarnitine was found to be the most promising lipid signature for both the diagnosis and prognosis of critically ill patients, with accuracies of 75% for both purposes. In short, we presented the determination of lipid signatures as a potential tool for differential diagnosis of sepsis and SIRS and prognosis of these patients.
Keywords: SIRS; lipidomics; multivariate analysis; sepsis.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures



References
-
- Singer M., Deutschman C.S., Seymour C., Shankar-Hari M., Annane D., Bauer M., Bellomo R., Bernard G.R., Chiche J.D., Coopersmith C.M., et al. The third international consensus definitions for sepsis and septic shock (sepsis-3) JAMA J. Am. Med. Assoc. 2016;315:801–810. doi: 10.1001/jama.2016.0287. - DOI - PMC - PubMed
-
- Shankar-Hari M., Harrison D.A., Rowan K.M. Differences in Impact of Definitional Elements on Mortality Precludes International Comparisons of Sepsis Epidemiology—A Cohort Study Illustrating the Need for Standardized Reporting. Crit. Care Med. 2016;44:2223–2230. doi: 10.1097/CCM.0000000000001876. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
