

Digital Training for Non-Specialist Health Workers to Deliver a Brief Psychological Treatment for Depression in Primary Care in India: Findings from a Randomized Pilot Study
- PMID: 32883018
- PMCID: PMC7503742
- DOI: 10.3390/ijerph17176368
Digital Training for Non-Specialist Health Workers to Deliver a Brief Psychological Treatment for Depression in Primary Care in India: Findings from a Randomized Pilot Study
Abstract
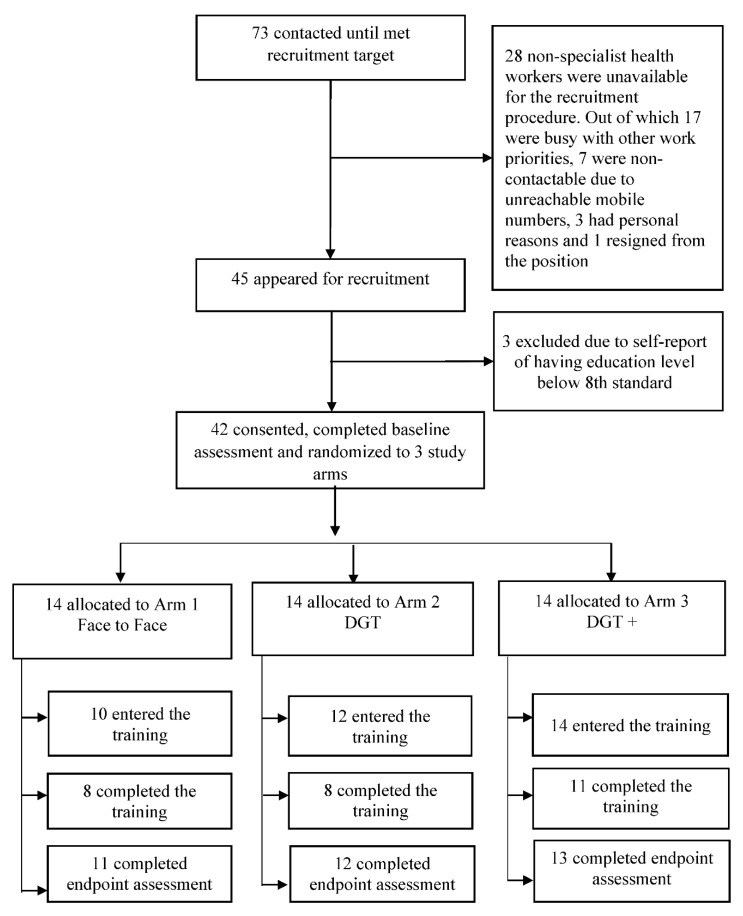
Introduction: Task sharing holds promise for scaling up depression care in countries such as India, yet requires training large numbers of non-specialist health workers. This pilot trial evaluated the feasibility and acceptability of a digital program for training non-specialist health workers to deliver a brief psychological treatment for depression. Methods: Participants were non-specialist health workers recruited from primary care facilities in Sehore, a rural district in Madhya Pradesh, India. A three-arm randomized controlled trial design was used, comparing digital training alone (DGT) to digital training with remote support (DGT+), and conventional face-to-face training. The primary outcome was the feasibility and acceptability of digital training programs. Preliminary effectiveness was explored as changes in competency outcomes, assessed using a self-reported measure covering the specific knowledge and skills required to deliver the brief psychological treatment for depression. Outcomes were collected at pre-training and post-training. Results: Of 42 non-specialist health workers randomized to the training programs, 36 including 10 (72%) in face-to-face, 12 (86%) in DGT, and 14 (100%) in DGT+ arms started the training. Among these participants, 27 (64%) completed the training, with 8 (57%) in face-to-face, 8 (57%) in DGT, and 11 (79%) in DGT+. The addition of remote telephone support appeared to improve completion rates for DGT+ participants. The competency outcome improved across all groups, with no significant between-group differences. However, face-to-face and DGT+ participants showed greater improvement compared to DGT alone. There were numerous technical challenges with the digital training program such as poor connectivity, smartphone app not loading, and difficulty navigating the course content-issues that were further emphasized in follow-up focus group discussions with participants. Feedback and recommendations collected from participants informed further modifications and refinements to the training programs in preparation for a forthcoming large-scale effectiveness trial. Conclusions: This study adds to mounting efforts aimed at leveraging digital technology to increase the availability of evidence-based mental health services in primary care settings in low-resource settings.
Keywords: depression; digital technology; mental health; non-specialist health worker; pilot study; primary care; psychological treatment; task sharing; training.
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Digital training for non-specialist health workers to deliver a brief psychological treatment for depression in India: Protocol for a three-arm randomized controlled trial.Contemp Clin Trials. 2021 Mar;102:106267. doi: 10.1016/j.cct.2021.106267. Epub 2021 Jan 6. Contemp Clin Trials. 2021. PMID: 33421650
-
Design and Development of a Digital Program for Training Non-Specialist Health Workers to Deliver an Evidence-Based Psychological Treatment for Depression in Primary Care in India.J Technol Behav Sci. 2020 Dec;5(4):402-415. doi: 10.1007/s41347-020-00154-7. Epub 2020 Aug 31. J Technol Behav Sci. 2020. PMID: 34150992 Free PMC article.
-
Acceptability and feasibility of digital technology for training community health workers to deliver brief psychological treatment for depression in rural India.Asian J Psychiatr. 2019 Oct;45:99-106. doi: 10.1016/j.ajp.2019.09.006. Epub 2019 Sep 7. Asian J Psychiatr. 2019. PMID: 31557716 Free PMC article.
-
Telephone interventions for symptom management in adults with cancer.Cochrane Database Syst Rev. 2020 Jun 2;6(6):CD007568. doi: 10.1002/14651858.CD007568.pub2. Cochrane Database Syst Rev. 2020. PMID: 32483832 Free PMC article.
-
Digital Technology for Building Capacity of Nonspecialist Health Workers for Task Sharing and Scaling Up Mental Health Care Globally.Harv Rev Psychiatry. 2019 May/Jun;27(3):181-192. doi: 10.1097/HRP.0000000000000217. Harv Rev Psychiatry. 2019. PMID: 30958400 Free PMC article. Review.
Cited by
-
Data Science in Healthcare: COVID-19 and Beyond.Int J Environ Res Public Health. 2022 Mar 16;19(6):3499. doi: 10.3390/ijerph19063499. Int J Environ Res Public Health. 2022. PMID: 35329186 Free PMC article.
-
Coach-Supported Versus Self-guided Digital Training Course for a Problem-solving Psychological Intervention for Nonspecialists: Protocol for a Pre-Post Nested Randomized Controlled Trial.JMIR Res Protoc. 2023 Jun 13;12:e41981. doi: 10.2196/41981. JMIR Res Protoc. 2023. PMID: 37310781 Free PMC article.
-
A qualitative exploration of perceived needs and barriers of individuals with schizophrenia, caregivers and clinicians in using mental health applications in Madhya Pradesh, India.SSM Ment Health. 2022 Dec;2:100063. doi: 10.1016/j.ssmmh.2022.100063. SSM Ment Health. 2022. PMID: 36688236 Free PMC article.
-
Multi-sector determinants of implementation and sustainment for non-specialist treatment of depression and post-traumatic stress disorder in Kenya: a concept mapping study.Implement Sci Commun. 2025 May 7;6(1):55. doi: 10.1186/s43058-025-00744-7. Implement Sci Commun. 2025. PMID: 40336135 Free PMC article.
-
Adapting and deploying a digital program for training non-specialist providers on a brief psychological intervention for depression in rural Gujarat, India.PLOS Glob Public Health. 2024 Dec 5;4(12):e0003967. doi: 10.1371/journal.pgph.0003967. eCollection 2024. PLOS Glob Public Health. 2024. PMID: 39636831 Free PMC article.
References
-
- Sagar R., Dandona R., Gururaj G., Dhaliwal R., Singh A., Ferrari A., Dua T., Ganguli A., Varghese M., Chakma J.K. The burden of mental disorders across the states of India: The Global Burden of Disease Study 1990–2017. Lancet Psychiatry. 2020;7:148–161. doi: 10.1016/S2215-0366(19)30475-4. - DOI - PMC - PubMed
-
- Arvind B.A., Gururaj G., Loganathan S., Amudhan S., Varghese M., Benegal V., Rao G.N., Kokane A.M., Chavan B., Dalal P. Prevalence and socioeconomic impact of depressive disorders in India: Multisite population-based cross-sectional study. BMJ Open. 2019;9:e027250. doi: 10.1136/bmjopen-2018-027250. - DOI - PMC - PubMed
-
- Kokane A., Pakhare A., Gururaj G., Varghese M., Benegal V., Rao G.N., Arvind B., Shukla M., Mitra A., Yadav K. Healthcare. Multidisciplinary Digital Publishing Institute; Basel, Switzerland: 2019. Mental Health Issues in Madhya Pradesh: Insights from National Mental Health Survey of India 2016. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
