

Association Between 90-Minute Door-to-Balloon Time, Selective Exclusion of Myocardial Infarction Cases, and Access Site Choice: Insights From the Cardiac Care Outcomes Assessment Program (COAP) in Washington State
- PMID: 32883103
- PMCID: PMC9125502
- DOI: 10.1161/CIRCINTERVENTIONS.120.009179
Association Between 90-Minute Door-to-Balloon Time, Selective Exclusion of Myocardial Infarction Cases, and Access Site Choice: Insights From the Cardiac Care Outcomes Assessment Program (COAP) in Washington State
Abstract
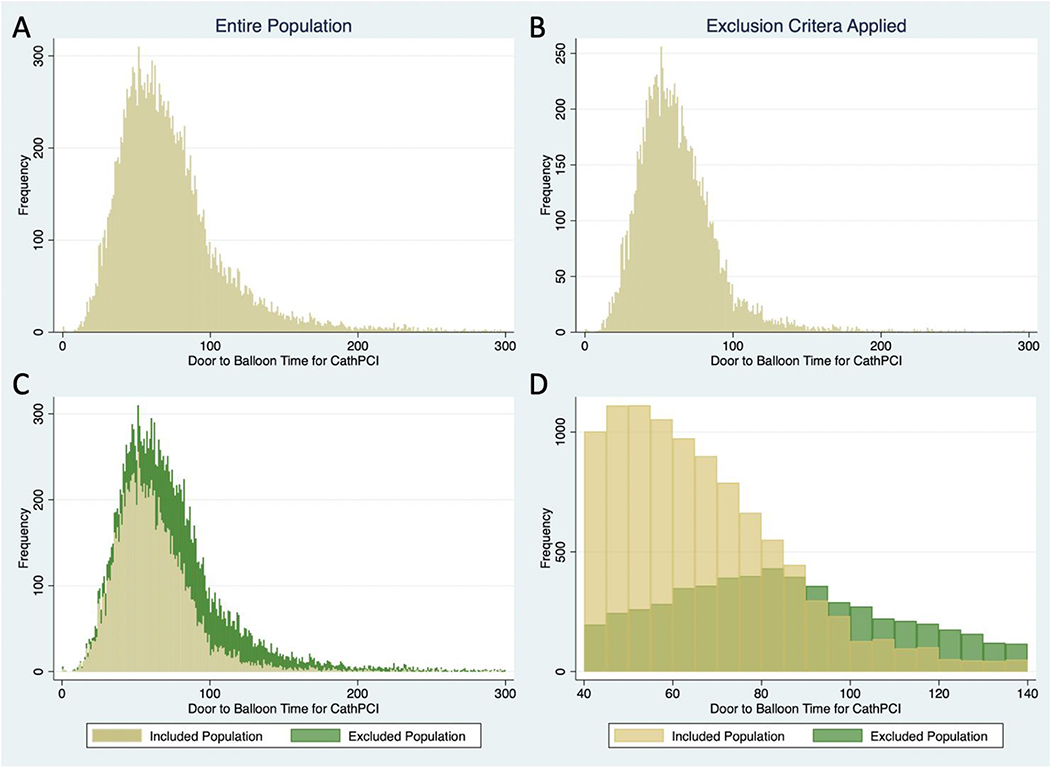
Background: For patients presenting with ST-segment-elevation myocardial infarction, national quality initiatives monitor hospitals' proportion of cases with door-to-balloon (D2B) time under 90 minutes. Hospitals are allowed to exclude patients from reporting and may modify behavior to improve performance. We sought to identify whether there is a discontinuity in the number of cases included in the D2B time metric at 90 minutes and whether operators were increasingly likely to pursue femoral access in patients with less time to meet the 90-minute quality metric.
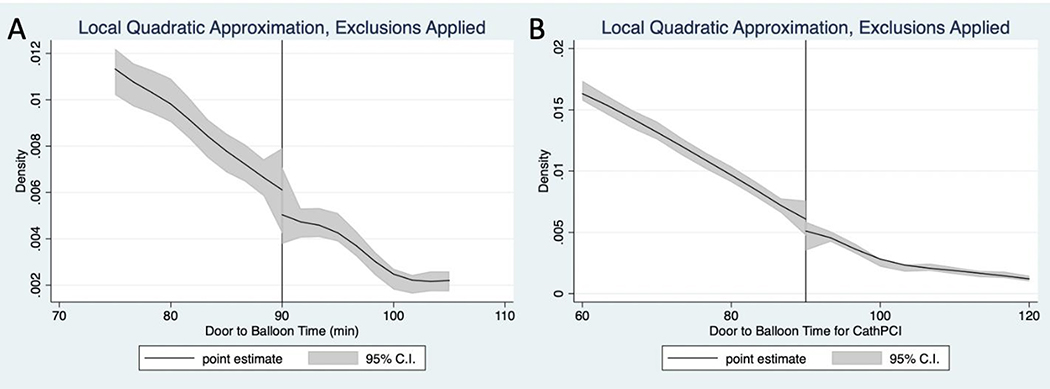
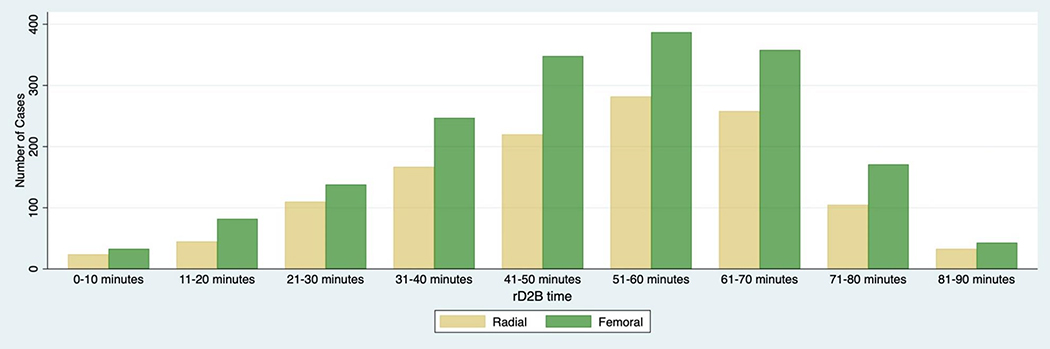
Methods: Adult patients with ST-segment-elevation myocardial infarction undergoing primary percutaneous coronary intervention from 2011 to 2018 were identified from the Cardiac Care Outcomes Assessment Program, a quality improvement registry in Washington state. We used the regression discontinuity framework to test for discontinuity at 90 minutes among the included cases. We defined a novel variable, remaining D2B as 90 minutes minus the time between hospital arrival and catheterization laboratory arrival. We estimated multivariable logistic regression models to assess the relationship between remaining D2B time and access site.
Results: A total of 19 348 patients underwent primary percutaneous coronary intervention and were included in the analysis. Overall, 7436 (38.4%) were excluded from the metric. There appeared to be a visual discontinuity in included cases around 90 minutes; however, local quadratic regression around the 90-minute cutoff did not reveal evidence of a significant discontinuity (P=0.66). Multivariable analysis showed no significant relationship between remaining D2B time and the odds of undergoing femoral access (P=0.73).
Conclusions: Among patients undergoing percutaneous coronary intervention for ST-segment-elevation myocardial infarction, we did not find evidence of a statistically significant discontinuity in the frequency of included cases around 90 minutes or an increased preference for femoral access correlated with decreasing time to meet the 90-minute D2B time quality metric. Together, these findings indicate no evidence of widespread inappropriate methods to improve performance on D2B time metrics.
Keywords: association; catheterization; hospitals; myocardial infarction; percutaneous coronary intervention.
Figures
Comment in
-
Using Discontinuity to Cross the Quality Chasm.Circ Cardiovasc Interv. 2020 Sep;13(9):e009887. doi: 10.1161/CIRCINTERVENTIONS.120.009887. Epub 2020 Sep 4. Circ Cardiovasc Interv. 2020. PMID: 32883105 No abstract available.
Similar articles
-
Prognostic Implications of Door-to-Balloon Time and Onset-to-Door Time on Mortality in Patients With ST -Segment-Elevation Myocardial Infarction Treated With Primary Percutaneous Coronary Intervention.J Am Heart Assoc. 2019 May 7;8(9):e012188. doi: 10.1161/JAHA.119.012188. J Am Heart Assoc. 2019. PMID: 31041869 Free PMC article.
-
Incremental Prognostic Value of Guideline-Directed Medical Therapy, Transradial Access, and Door-to-Balloon Time on Outcomes in ST-Segment-Elevation Myocardial Infarction.Circ Cardiovasc Interv. 2019 Mar;12(3):e007101. doi: 10.1161/CIRCINTERVENTIONS.118.007101. Circ Cardiovasc Interv. 2019. PMID: 30871354
-
Association of adoption of transradial access for percutaneous coronary intervention in ST elevation myocardial infarction with door-to-balloon time.Catheter Cardiovasc Interv. 2020 Aug;96(2):E165-E173. doi: 10.1002/ccd.28785. Epub 2020 Feb 27. Catheter Cardiovasc Interv. 2020. PMID: 32105411 Free PMC article.
-
Radial versus femoral access for primary percutaneous interventions in ST-segment elevation myocardial infarction patients: a meta-analysis of randomized controlled trials.JACC Cardiovasc Interv. 2013 Aug;6(8):814-23. doi: 10.1016/j.jcin.2013.04.010. JACC Cardiovasc Interv. 2013. PMID: 23968700 Review.
-
Update on primary PCI for patients with STEMI.Trends Cardiovasc Med. 2017 Feb;27(2):95-102. doi: 10.1016/j.tcm.2016.06.010. Epub 2016 Jun 27. Trends Cardiovasc Med. 2017. PMID: 27450063 Review.
Cited by
-
Cardiac rupture after ST-elevation myocardial infarction (STEMI): a 'Stitch' in time?J Thorac Dis. 2022 Jul;14(7):2454-2457. doi: 10.21037/jtd-22-720. J Thorac Dis. 2022. PMID: 35928626 Free PMC article. No abstract available.
-
Impact of the COVID-19 Pandemic on Patient Delay and Clinical Outcomes for Patients With Acute Myocardial Infarction.J Korean Med Sci. 2022 May 30;37(21):e167. doi: 10.3346/jkms.2022.37.e167. J Korean Med Sci. 2022. PMID: 35638194 Free PMC article.
-
Burnout of Support Personnel in the Cardiac Catheterization Laboratory.Cardiol Res. 2022 Oct;13(5):283-288. doi: 10.14740/cr1439. Epub 2022 Oct 25. Cardiol Res. 2022. PMID: 36405231 Free PMC article.
-
Integrating mixed reality preparation into acute coronary syndrome simulation for nursing students: a single-group pretest-posttest study.BMC Nurs. 2024 Jul 9;23(1):468. doi: 10.1186/s12912-024-02110-9. BMC Nurs. 2024. PMID: 38982463 Free PMC article.
-
Analysis of the Weekend Effect on Mortality, Diagnostic Coronary Angiography, and Percutaneous Coronary Intervention in Acute Myocardial Infarction Across Rural US Hospitals.Cureus. 2024 Feb 7;16(2):e53751. doi: 10.7759/cureus.53751. eCollection 2024 Feb. Cureus. 2024. PMID: 38465191 Free PMC article.
References
-
- McNamara RL, Wang Y, Herrin J, et al. Effect of door-to-balloon time on mortality in patients with ST-segment elevation myocardial infarction. J Am Coll Cardiol. 2006;47:2180–2186. - PubMed
-
- Berger PB, Ellis SG, Holmes DR Jr, Granger CB, Criger DA, Betriu A, Topol EJ, Califf RM. Relationship between delay in performing direct coronary angioplasty and early clinical outcome in patients with acute myocardial infarction: results from the global use of strategies to open occluded arteries in Acute Coronary Syndromes (GUSTO-IIb) trial. Circulation. 1999;100:14–20. - PubMed
-
- O’Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;61:e78–e140. - PubMed
-
- Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39:119–177. - PubMed
-
- Nallamothu BK, Wang Y, Bradley EH, Ho KK, Curtis JP, Rumsfeld JS, Masoudi FA, Krumholz HM. Comparing hospital performance in door-to-balloon time between the Hospital Quality Alliance and the National Cardiovascular Data Registry. J Am Coll Cardiol. 2007;50:1517–1519. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
