

Coronary Computed Tomography Angiography From Clinical Uses to Emerging Technologies: JACC State-of-the-Art Review
- PMID: 32883417
- PMCID: PMC7480405
- DOI: 10.1016/j.jacc.2020.06.076
Coronary Computed Tomography Angiography From Clinical Uses to Emerging Technologies: JACC State-of-the-Art Review
Abstract
Evaluation of coronary artery disease (CAD) using coronary computed tomography angiography (CCTA) has seen a paradigm shift in the last decade. Evidence increasingly supports the clinical utility of CCTA across various stages of CAD, from the detection of early subclinical disease to the assessment of acute chest pain. Additionally, CCTA can be used to noninvasively quantify plaque burden and identify high-risk plaque, aiding in diagnosis, prognosis, and treatment. This is especially important in the evaluation of CAD in immune-driven conditions with increased cardiovascular disease prevalence. Emerging applications of CCTA based on hemodynamic indices and plaque characterization may provide personalized risk assessment, affect disease detection, and further guide therapy. This review provides an update on the evidence, clinical applications, and emerging technologies surrounding CCTA as highlighted at the 2019 National Heart, Lung and Blood Institute CCTA Summit.
Keywords: atherosclerosis; coronary artery disease; coronary computed tomography angiography.
Published by Elsevier Inc.
Figures

References
-
- Knuuti J, Wijns W, Saraste A et al. 2019. ESC Guidelines for the diagnosis and management of chronic coronary syndromesThe Task Force for the diagnosis and management of chronic coronary syndromes of the European Society of Cardiology (ESC). Eur Heart J.
-
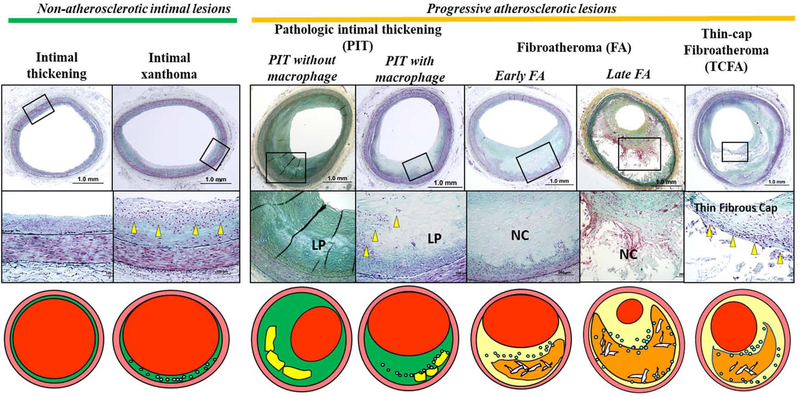
- Yahagi K, Kolodgie FD, Otsuka F et al. Pathophysiology of native coronary, vein graft, and in-stent atherosclerosis. Nat Rev Cardiol 2016;13:79–98. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
