

Transcranial MR Imaging-Guided Focused Ultrasound Interventions Using Deep Learning Synthesized CT
- PMID: 32883668
- PMCID: PMC7661089
- DOI: 10.3174/ajnr.A6758
Transcranial MR Imaging-Guided Focused Ultrasound Interventions Using Deep Learning Synthesized CT
Abstract
Background and purpose: Transcranial MR imaging-guided focused ultrasound is a promising novel technique to treat multiple disorders and diseases. Planning for transcranial MR imaging-guided focused ultrasound requires both a CT scan for skull density estimation and treatment-planning simulation and an MR imaging for target identification. It is desirable to simplify the clinical workflow of transcranial MR imaging-guided focused ultrasound treatment planning. The purpose of this study was to examine the feasibility of deep learning techniques to convert MR imaging ultrashort TE images directly to synthetic CT of the skull images for use in transcranial MR imaging-guided focused ultrasound treatment planning.
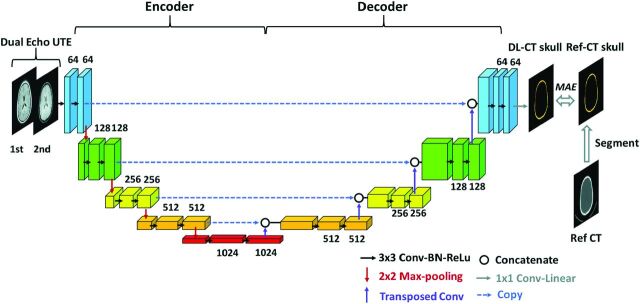
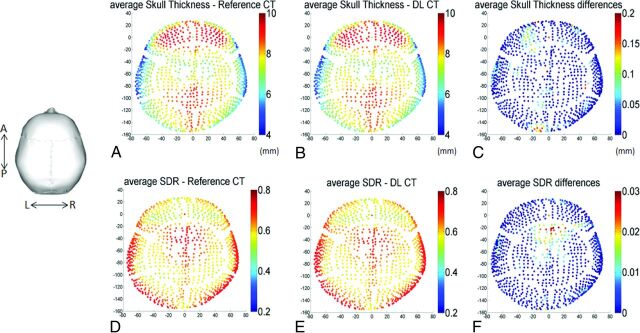
Materials and methods: The U-Net neural network was trained and tested on data obtained from 41 subjects (mean age, 66.4 ± 11.0 years; 15 women). The derived neural network model was evaluated using a k-fold cross-validation method. Derived acoustic properties were verified by comparing the whole skull-density ratio from deep learning synthesized CT of the skull with the reference CT of the skull. In addition, acoustic and temperature simulations were performed using the deep learning CT to predict the target temperature rise during transcranial MR imaging-guided focused ultrasound.
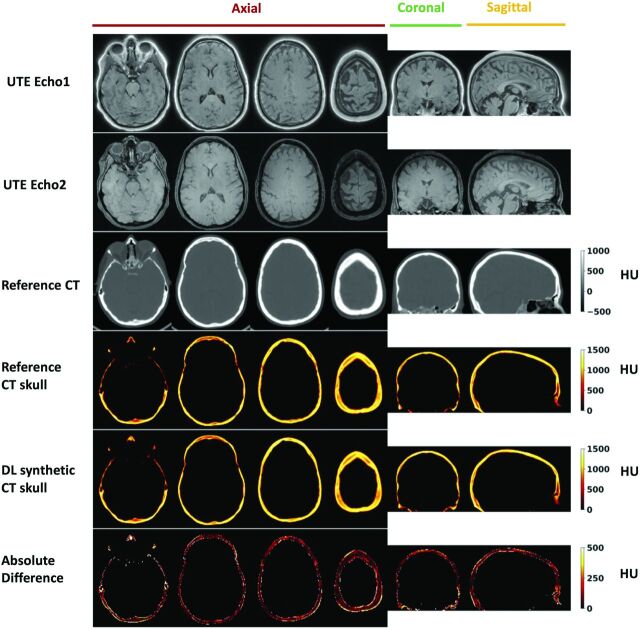
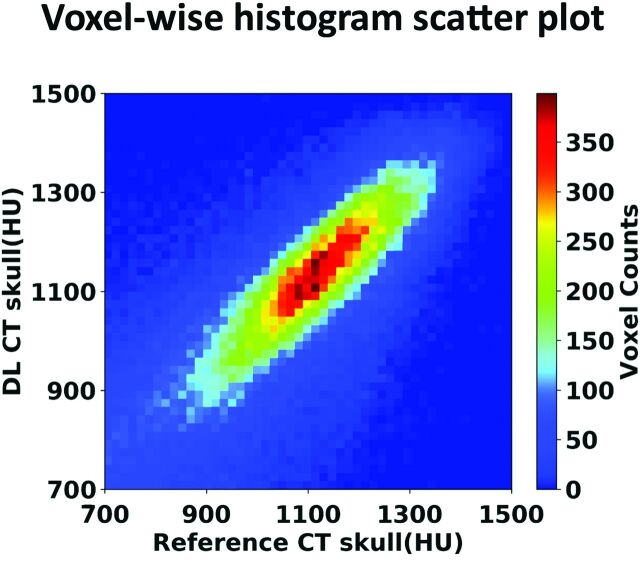
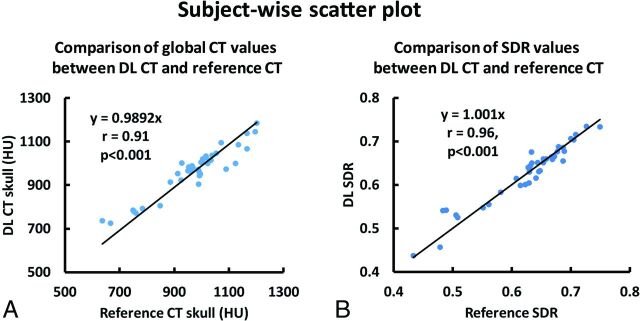
Results: The derived deep learning model generates synthetic CT of the skull images that are highly comparable with the true CT of the skull images. Their intensities in Hounsfield units have a spatial correlation coefficient of 0.80 ± 0.08, a mean absolute error of 104.57 ± 21.33 HU, and a subject-wise correlation coefficient of 0.91. Furthermore, deep learning CT of the skull is reliable in the skull-density ratio estimation (r = 0.96). A simulation study showed that both the peak target temperatures and temperature distribution from deep learning CT are comparable with those of the reference CT.
Conclusions: The deep learning method can be used to simplify workflow associated with transcranial MR imaging-guided focused ultrasound.
© 2020 by American Journal of Neuroradiology.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical