

Haemodynamic analysis of adult patients with moyamoya disease: CT perfusion and DSA gradings
- PMID: 32883875
- PMCID: PMC8005907
- DOI: 10.1136/svn-2019-000317
Haemodynamic analysis of adult patients with moyamoya disease: CT perfusion and DSA gradings
Abstract
Object: Moyamoya disease (MMD) is a common and chronic progressive stenotic-occlusive cerebrovascular disease in Eastern Asia. To evaluate the hemispheric haemodynamic status of adult patients with MMD, we explored the potential risk factors of hemispheric perfusion alterations with CT perfusion (CTP) and DSA.
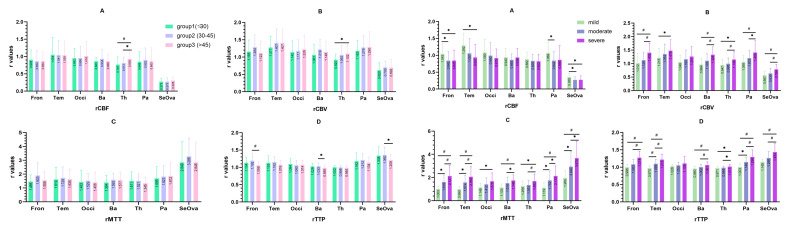
Methods: We retrospectively reviewed 44 male and 44 female (176 hemispheres) adult patients with MMD who had both DSA and CTP. Data on cerebral blood perfusion (CBF), cerebral blood volume (CBV), mean transmit time (MTT), time to peak (TTP) of cerebral hemisphere and cerebellum were gathered and difference of relative haemodynamic parameters between different subgroups were assessed with independent sample t analysis, one-way analysis of variance and general linear regression analysis.
Results: Parameters in regional CBF (rCBF) of frontal, temporal lobe and basal ganglia in female was more superior than male. rCBF, regional MTT (rMTT) and regional TTP (rTTP) in adult MMD patients with haemorrhage were superior than the ischaemic. With the increase of age, significant difference could be seen in rCBF and rCBV of thalamus. However, with progress of arterial stenosis, significant difference could only be obsevrved in rCBV, rMTT and rTTP, whereas rCBF had no significant difference. For increase of moyamoya vessels, significant decrease of rCBF could be seen in temporal and parietal lobe. With the increase of compensatory artery numbers, no significant difference could be seen in rCBF parameters (p>0.05).
Conclusions: In adult MMD patients, age, gender and clinical type were potential risk factors for the change of cerebral perfusion. When arterial stenosis is worsened, moyamoya vessels could alter perfusion of temporal and parietal lobe, but not frontal lobe. Extracranial/intracranial compensatory arteries could maintain microcirculation stability in frontal lobe and basal ganglia, indicating that the protection from extracranial compensatory arteries, a theoretic base for surgery treatment if necessary.
Keywords: CT perfusion; angiography; blood flow; hemorrhage; stroke.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures




References
MeSH terms
LinkOut - more resources
Full Text Sources