

Association of TDP-43 proteinopathy, cerebral amyloid angiopathy, and Lewy bodies with cognitive impairment in individuals with or without Alzheimer's disease neuropathology
- PMID: 32883971
- PMCID: PMC7471113
- DOI: 10.1038/s41598-020-71305-2
Association of TDP-43 proteinopathy, cerebral amyloid angiopathy, and Lewy bodies with cognitive impairment in individuals with or without Alzheimer's disease neuropathology
Abstract
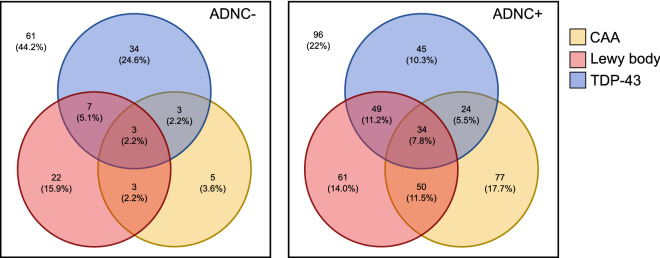
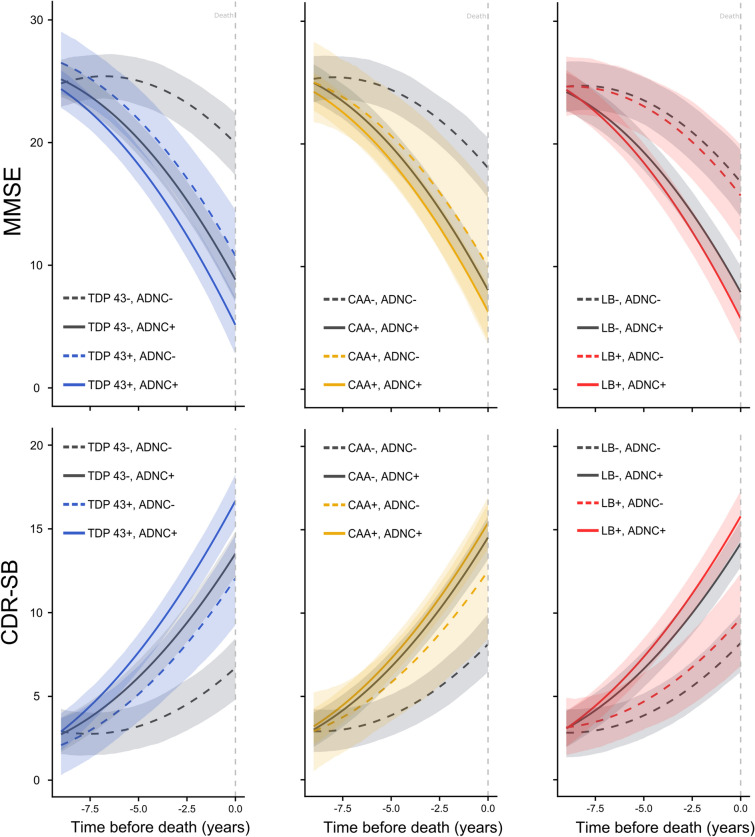
Alzheimer's disease patients typically present with multiple co-morbid neuropathologies at autopsy, but the impact of these pathologies on cognitive impairment during life is poorly understood. In this study, we developed cognitive trajectories for patients with common co-pathologies in the presence and absence of Alzheimer's disease neuropathology. Cognitive trajectories were modelled in a Bayesian hierarchical regression framework to estimate the effects of each neuropathology on cognitive decline as assessed by the mini-mental state examination and the clinical dementia rating scale sum of boxes scores. We show that both TDP-43 proteinopathy and cerebral amyloid angiopathy associate with cognitive impairment of similar magnitude to that associated with Alzheimer's disease neuropathology. Within our study population, 63% of individuals given the 'gold-standard' neuropathological diagnosis of Alzheimer's disease in fact possessed either TDP-43 proteinopathy or cerebral amyloid angiopathy of sufficient severity to independently explain the majority of their cognitive impairment. This suggests that many individuals diagnosed with Alzheimer's disease may actually suffer from a mixed dementia, and therapeutics targeting only Alzheimer's disease-related processes may have severely limited efficacy in these co-morbid populations.
Conflict of interest statement
Prof Roy M. Anderson completed 10 years as a Non-Executive director of GlaxoSmithKline (GSK) in June 2019. GSK played no part in this research, its funding or the preparation of the manuscript. Prof John Collinge is a shareholder and Director of D-Gen Limited, an academic spin-out company working in the field of prion disease diagnosis, decontamination and therapeutics. The remaining authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
- P50 AG005142/AG/NIA NIH HHS/United States
- P30 AG010133/AG/NIA NIH HHS/United States
- P50 AG005146/AG/NIA NIH HHS/United States
- P50 AG047266/AG/NIA NIH HHS/United States
- P30 AG008017/AG/NIA NIH HHS/United States
- P50 AG025688/AG/NIA NIH HHS/United States
- P50 AG005133/AG/NIA NIH HHS/United States
- P50 AG005138/AG/NIA NIH HHS/United States
- P50 AG047366/AG/NIA NIH HHS/United States
- P30 AG019610/AG/NIA NIH HHS/United States
- MR/L023784/2/MRC_/Medical Research Council/United Kingdom
- P30 AG028383/AG/NIA NIH HHS/United States
- P30 AG013854/AG/NIA NIH HHS/United States
- P30 AG053760/AG/NIA NIH HHS/United States
- P30 AG062428/AG/NIA NIH HHS/United States
- P30 AG010124/AG/NIA NIH HHS/United States
- P50 AG023501/AG/NIA NIH HHS/United States
- P30 AG062421/AG/NIA NIH HHS/United States
- P30 AG035982/AG/NIA NIH HHS/United States
- P50 AG008702/AG/NIA NIH HHS/United States
- U01 AG016976/AG/NIA NIH HHS/United States
- P30 AG008051/AG/NIA NIH HHS/United States
- P50 AG005681/AG/NIA NIH HHS/United States
- P30 AG013846/AG/NIA NIH HHS/United States
- MC_UP_1604/1/MRC_/Medical Research Council/United Kingdom
- P50 AG047270/AG/NIA NIH HHS/United States
- P30 AG062429/AG/NIA NIH HHS/United States
- P50 AG005136/AG/NIA NIH HHS/United States
- P30 AG049638/AG/NIA NIH HHS/United States
- P30 AG012300/AG/NIA NIH HHS/United States
- P30 AG062422/AG/NIA NIH HHS/United States
- P50 AG016573/AG/NIA NIH HHS/United States
- P30 AG010161/AG/NIA NIH HHS/United States
- MR/R015600/1/MRC_/Medical Research Council/United Kingdom
- P30 AG062715/AG/NIA NIH HHS/United States
- P30 AG066468/AG/NIA NIH HHS/United States
- P30 AG010129/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
