

Towards personalized induction therapy for esophageal adenocarcinoma: organoids derived from endoscopic biopsy recapitulate the pre-treatment tumor
- PMID: 32884042
- PMCID: PMC7471705
- DOI: 10.1038/s41598-020-71589-4
Towards personalized induction therapy for esophageal adenocarcinoma: organoids derived from endoscopic biopsy recapitulate the pre-treatment tumor
Abstract
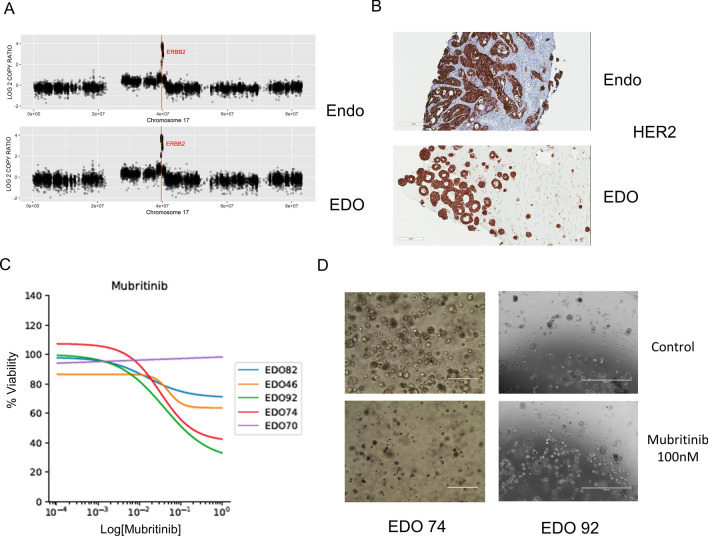
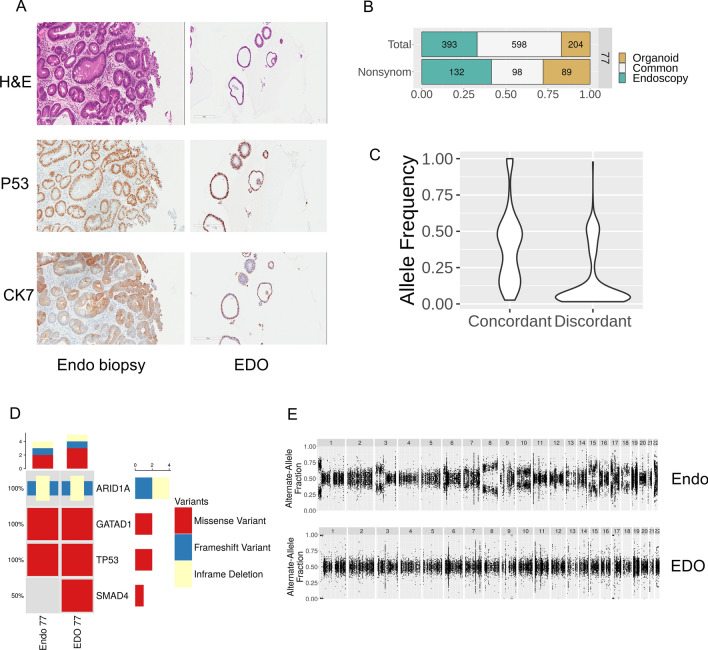
Esophageal adenocarcinoma has few known recurrent mutations and therefore robust, reliable and reproducible patient-specific models are needed for personalized treatment. Patient-derived organoid culture is a strategy that may allow for the personalized study of esophageal adenocarcinoma and the development of personalized induction therapy. We therefore developed a protocol to establish EAC organoids from endoscopic biopsies of naïve esophageal adenocarcinomas. Histologic characterization and molecular characterization of organoids by whole exome sequencing demonstrated recapitulation of the tumors' histology and genomic (~ 60% SNV overlap) characteristics. Drug testing using clinically appropriate chemotherapeutics and targeted therapeutics showed an overlap between the patient's tumor response and the corresponding organoids' response. Furthermore, we identified Barrett's esophagus epithelium as a potential source of organoid culture contamination. In conclusion, organoids can be robustly cultured from endoscopic biopsies of esophageal adenocarcinoma and recapitulate the originating tumor. This model demonstrates promise as a tool to better personalize therapy for esophageal adenocarcinoma patients.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Al-Batran, S.E. et al. The RENAISSANCE (AIO-FLOT5) trial: Effect of chemotherapy alone vs. chemotherapy followed by surgical resection on survival and quality of life in patients with limited-metastatic adenocarcinoma of the stomach or esophagogastric junction—a phase III trial of the German AIO/CAO-V/CAOGI. BMC Cancer17, 893 (2017). - PMC - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
